
Coenzymated Methyl B-12 Vitamin
Despite its critical role in health and longevity, vitamin B-12 is one of the most overlooked essential nutrients by both the public and medical professionals. It supports cell division and repair, helps prevent anemia and cancer, regulates hormones, and protects sleep, mood, memory, nerves, hearing, vision, heart, and brain function. It also plays an important role in appetite control, weight regulation, energy levels, and fertility.
For these and many other reasons listed below, top celebrities like Madonna, Rihanna, Katy Perry, Charlize Theron, Simon Cowell, and Hugh Jackman, as well as leading athletes, politicians, and CEOs, have been getting weekly B-12 injections costing up to $250 per shot since the early 1950s. You can now get the same benefits with sublingual tablets and results that are just as good or better. My wife Tatyana and I have been doing exactly that since 1996, and with remarkable outcomes.
I also believe B-12 deficiency plays a major role in the 1,000-fold rise of autism in children since the 1930s and the explosion of dementia in older adults. Because B-12 is required for DNA synthesis, it may also contribute significantly to the alarming rise in cancer rates among children and younger adults.
You can also add to those three disasters above the obesity epidemic, memory loss, heart disease and stroke, chronic fatigue, depression, weakened immunity, pernicious anemia, infertility, erectile dysfunction, inflammatory bowel disease (IBD), Alzheimer's and Parkinson's diseases, and premature aging.
I don’t like preaching or fear-mongering, but if you ignore this dirt-cheap supplement (less than $0.30 a day), you’re playing Russian roulette with not one, but five bullets in the chamber, and here is why:

Vitamin B-12 is found almost exclusively in animal-derived foods, primarily organ meats, shellfish, red meat, eggs, and dairy. Unlike other vitamins, it is not present in plants unless they are contaminated with bacteria that produce B-12 or artificially fortified.
Even in omnivorous diets, absorption depends on multiple steps: sufficient stomach acid to release B-12 from protein, a functioning pancreas to supply enzymes, a healthy small intestine to produce intrinsic factor, and intact receptors in the ileum to complete uptake.
Any disruption along this chain is common in older adults, people with low stomach acid, users of acid-suppressing drugs, or those with intestinal inflammation, and can drastically reduce absorption, making dietary intake alone unreliable, even when consumption appears sufficient.
| |||||||||
| |||||||||
Vitamin B-12 absorption requires a specialized transport protein called intrinsic factor. The factor name sounds vague because scientists originally had no idea what it was, only that something inside the body was essential for B-12 assimilation. It was later discovered that it is a glycoprotein secreted by the stomach’s parietal cells.
Once B-12 is freed from food by stomach acid and enzymes, an intrinsic factor binds to it and escorts it through the small intestine to the terminal ileum, where the complex is finally absorbed. Without the intrinsic factor, even large amounts of dietary or supplemental B-12 will pass through the gut unused.
The production of intrinsic factor is not constant. When you eat a protein-rich meal, the stomach responds by secreting both hydrochloric acid and digestive enzymes, along with intrinsic factor. Low-protein diets, prolonged fasting, or chronic use of acid-suppressing drugs (such as PPIs or H2 blockers) can reduce this response, leading to insufficient intrinsic factor secretion. Over time, this can silently impair B-12 absorption, even if dietary intake appears adequate.
Individuals using GLP-1 drugs often experience delayed gastric emptying, reduced stomach acid production, and lower overall food intake. These changes reduce the secretion of intrinsic factor and limit the availability of B-12 in the gut. In this context, sublingual B-12 becomes essential because it bypasses the digestive system entirely.
Instead of relying on gastric acid and intestinal transport, sublingual tablets dissolve under the tongue and are absorbed directly into the bloodstream through the oral mucosa, making them far more reliable for maintaining B-12 status during GLP-1 therapy or other restrictive diets.
Advantages of methylcobalamin vs cyanocobalamin
Unlike this formula, most commercial B-12 supplements use cyanocobalamin, a synthetic form of B-12 bound to a cyanide molecule. It’s inexpensive, shelf-stable, and has been used for decades in fortified foods and multivitamins. However, it is not biologically active and must first be converted by the liver into either methylcobalamin or adenosylcobalamin — the two forms the body actually uses. This conversion is relatively inefficient and may be impaired in people with genetic polymorphisms (e.g., MTHFR), liver dysfunction, or chronic illness.
This formula uses methylcobalamin, a coenzymated form of B-12 already in its active state. It can enter cells and participate directly in methylation* and homocysteine metabolism without requiring conversion. Clinical studies suggest that methylcobalamin is better retained in tissues, especially in the central nervous system, and may be more effective for neurological repair and cognitive support. However, it is more expensive and less stable in multivitamin blends, which is why most mass-market supplements still rely on cyanocobalamin.
In practical terms, methylcobalamin offers superior bioavailability and safety, particularly for people with impaired detoxification, absorption issues, or neurological symptoms.
*Methylation is a chemical process where a methyl group (CH3) is added to a molecule. It plays a crucial role in regulating various biological processes, including development and disease.
Advantages of the sublingual tablets vs oral formulas
Most over-the-counter B-12 supplements come in swallowed tablet or capsule form. These rely on normal digestive function for absorption: adequate stomach acid to release B-12 from its binding, healthy secretion of intrinsic factor, and intact receptors in the terminal ileum (the very last section of the small intestine). Any disruption in this process, common with aging, acid-suppressing medications, bariatric surgery, and chronic GI disorders, can sharply reduce how well B-12 is absorbed.
Sublingual B-12 bypasses the digestive system entirely. The tablets dissolves under the tongue and is absorbed directly into the bloodstream through the oral mucosa. This route avoids dependence on stomach acid, intrinsic factor, and intestinal transport altogether, making it especially effective for individuals with compromised absorption or reduced dietary intake.
Studies show that sublingual B-12 provides greater systemic delivery compared to oral tablets and, in some cases, rivals the effectiveness of intramuscular injections (a technique for delivering medication deep into the muscles) without the need for medical supervision or needles. For people with low energy, neurological symptoms, or compromised intestinal function, sublingual B-12 is the more reliable, faster-acting, and substantially less expensive option.
Physiological functions and deficiency symptoms
Vitamin B-12 deficiency can take years to develop and often goes unnoticed until symptoms become serious or irreversible. Because B-12 is involved in so many critical systems — blood formation, nerve function, cognition — the signs of deficiency are often misdiagnosed or mistaken for aging, stress, and unrelated conditions. This section outlines the most common clinical uses of B-12 and the symptoms that may indicate a hidden deficiency:
-
Cell division and repair.Required for the production and repair of DNA during cell division, especially in rapidly dividing tissues such as the bone marrow and gastrointestinal lining. Deficiency slows DNA replication, leading to abnormal cell division and dysfunctional tissue maintenance.
Faulty or incomplete DNA replication increases the risk of mutations, chromosomal breakage, and missegregation during cell division. This instability is a known early feature in cancer development, although B-12 deficiency alone is not a confirmed carcinogen.
High-turnover tissues (i.e., the speed of cell replacement), like the gastrointestinal epithelium, become thin, fragile, and inflamed. These complications can present as glossitis (inflammation of the tongue), mouth ulcers, esophagitis, or intestinal malabsorption (apparent from bloating).
Cancer. B-12 deficiency may raise the risk of cancer by making DNA more prone to damage during cell division. It can also interfere with the control of genes that suppress tumors or prevent abnormal cell growth. These effects are especially likely to affect tissues with rapid turnover, such as the gastrointestinal lining and bone marrow, where mutations can accumulate faster.
Epidemiological studies have linked low B-12 levels to higher incidence of breast, cervical, colorectal, and hematologic cancers, although causality remains difficult to isolate due to overlapping deficiencies in folate and B-6. Still, maintaining adequate B-12 appears to be a low-cost, low-risk strategy for minimizing one of the modifiable risks of carcinogenesis.
Prevention of anemia.Vitamin B-12 plays a central role in red blood cell production by enabling proper DNA synthesis during cell division in the bone marrow. When B-12 is sufficient, immature red blood cells (erythroblasts) divide and mature into small, flexible, hemoglobin-rich cells capable of transporting oxygen efficiently.
B-12 deficiency leads to megaloblastic anemia, marked by large, fragile, oxygen-poor red cells. This condition leads to weakness, paleness, and breathlessness.
Distinguishing between iron-deficiency anemia and B-12-related anemia can be challenging because both conditions present similar symptoms—fatigue, weakness, pallor, and shortness of breath.
In mixed cases common in older adults, vegans, or individuals with chronic illnesses, the cell size may appear normal, masking the true cause. Without targeted testing, such as serum B-12, methylmalonic acid, homocysteine, and ferritin levels, misdiagnosis is easy, and inappropriate treatment can delay recovery or worsen symptoms.
-
Nerve, memory, and mood protection.Supports the synthesis and preservation of the myelin sheath that insulates nerves. A deficiency progressively damages peripheral and central nerves, resulting in numbness, tingling, burning, poor coordination, and, in severe cases, permanent neurological disability.
Chronic B-12 deficiency presents with cognitive changes, mood disturbances, and memory loss, making it difficult to distinguish from early dementia, multiple sclerosis, or chronic fatigue syndrome. Prolonged deficiency can result in permanent nerve damage even after B-12 levels are restored.
-
Heart and brain protection. Vitamin B-12, along with vitamins B-6 (pyridoxine) and Folate (B-9), acts as a cofactor for recycling homocysteine.With low B-12, homocysteine builds up in the bloodstream, a condition known as hyperhomocysteinemia.
Elevated homocysteine makes the arteries prone to inflammation, stiffness, and damage, increasing the risk of atherosclerosis, heart attacks, and strokes. It is also linked to blood clots, poor circulation, and pregnancy complications, including neural tube defects.
-
Mood and cognitive function.B-12 is involved in the synthesis of serotonin, dopamine, and other mood-regulating neurotransmitters. Deficiency may result in depression, anxiety, irritability, memory loss, and, in older adults, may contribute to dementia-like syndromes.
In some cases, these symptoms appear long before megaloblastic anemia or neurological signs, making the deficiency easy to miss. Studies have linked low B-12 status to an increased risk of major depressive disorder, cognitive impairment, and age-related brain atrophy, even in people with normal blood counts.
Because B-12 also supports methylation and reduces homocysteine—both critical for brain function—its deficiency can impair mood stability, stress resilience, and executive function, particularly under chronic psychological or metabolic stress.
-
Energy metabolism.B-12 facilitates the conversion of fatty acids and amino acids into the primary energy source for all cells. When B-12 is deficient, this process slows down, starving cells of energy and forcing the body to rely on less efficient metabolic pathways. The result is persistent fatigue, muscle weakness, poor physical endurance, and difficulty recovering from physical or mental exertion. This lack of cellular energy also affects brain functionality, which has extremely high metabolic demands.
Over time, B-12 deficiency can lead to mental fatigue, reduced alertness, brain fog, and decreased motivation, often compounding the emotional symptoms described in the previous section. What may feel like depression, apathy, or burnout is sometimes a direct result of impaired mitochondrial energy production driven by a slow and silent decline in B-12 status.
-
Hormonal and cellular support. Vitamin B-12 plays a key role in a process called methylation. It is required for making neurotransmitters like serotonin and dopamine, breaking down hormones like estrogen, and neutralizing toxins in the liver. B-12 deficiency slows down methylation and leads to problems with mood, memory, hormone balance, fertility, libido, immune function, and liver detoxification. Over time, poor methylation contributes to chronic inflammation, cellular stress, and accelerated aging.
-
Prevention of obesity. Low B-12 status is common in people with obesity, even among those who consume animal products. Overweight individuals commonly have higher circulating levels of homocysteine, a known marker of B-12 deficiency, which has also been linked to insulin resistance, visceral fat accumulation, and poor glucose control.
B-12 is also involved in mitochondrial energy metabolism and fatty acid processing. When B-12 is deficient, fatty acids are not efficiently converted into energy. Instead, they're more likely to be stored as fat.
Safe weight loss. During weight loss, especially when calories or protein intake are reduced, the demand for B-12 increases while intake often declines. This situation is particularly true for people using GLP-1 drugs, intermittent fasting, or restrictive diets. All of these suppress appetite and reduce total food intake, which in turn lowers B-12 intake and secretion of intrinsic factor needed for absorption.
At the same time, the body is attempting to mobilize stored fat and maintain lean mass, both of which depend on efficient mitochondrial function. B-12 plays a direct role in this process through its involvement in the Krebs cycle, which enables the conversion of amino acids and fatty acids into ATP. When B-12 is lacking, patients often report fatigue, poor exercise tolerance, slow recovery, and cognitive decline. These symptoms can derail weight loss efforts or create rebound cycles because of overeating and inactivity.
Appetite regulation. B-12 is essential for synthesizing serotonin and dopamine, essential neurotransmitters which influence appetite, impulse control, and satiety. Deficiency in B-12 has been associated with mood instability, increased emotional eating, and altered hunger signaling, particularly in individuals already predisposed to compulsive eating patterns.
Low B-12 levels can blunt appetite completely, leading to undernutrition. In adults with stress-related or reward-driven eating patterns, low B-12 may reduce the brain's ability to regulate desire for calorie-dense foods, especially under metabolic stress. While B-12 doesn't act as a direct appetite suppressant, its role in neurological balance makes it a critical background factor in any attempt to stabilize eating behavior over time.
Sleep regulation. Vitamin B-12 plays a supporting role in regulating circadian rhythms, the internal 24-hour clock that controls when we feel alert and when we feel sleepy. One of its key functions is assisting in the synthesis of melatonin, the hormone that signals the body to prepare for sleep. This process depends on methylation, which in turn depends on adequate B-12.
A deficiency in B-12 can disrupt this cycle. Some people experience delayed sleep onset, poor sleep quality, or early waking that doesn't resolve with standard sleep hygiene. Others report feeling chronically tired during the day but wired or restless at night. These symptoms reflect real biochemical disruptions in how the brain transitions between wakefulness and rest.
Low B-12 is also linked to reduced serotonin production, which affects both mood and sleep initiation. Since serotonin is a precursor to melatonin, a drop in serotonin can indirectly disturb sleep patterns. That is why people with B-12 deficiency often describe feeling mentally fatigued but unable to rest, even when exhausted.
Supplementation with B-12, especially in active, sublingual form, has been reported in some studies and clinical observations to help restore more stable sleep cycles, particularly in older adults or individuals recovering from long periods of stress, malnutrition, or disordered eating.
While B-12 is not a sedative and doesn't induce sleep directly, it helps maintain the neurological balance required for consistent, restorative sleep. Without it, even the best sleep protocols often fall short.
Hearing loss protection. Vitamin B-12 deficiency has been linked to sensorineural hearing loss, particularly in older adults. The cochlea and auditory nerve require adequate B-12 to maintain the myelin sheath and protect against oxidative and vascular damage. Several studies have shown that individuals with low B-12 have a higher risk of age-related hearing decline, tinnitus, and noise-induced hearing loss.
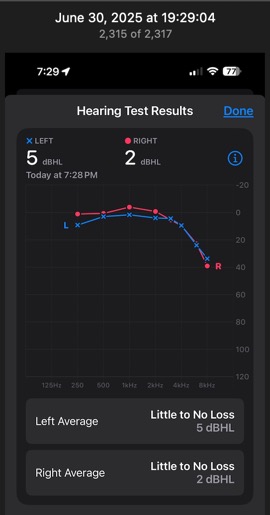
To check my own hearing objectively, I used the hearing test built into the iPhone for AirPods Pro. It’s designed to approximate clinical-grade testing and is often comparable to what ENT specialists use for screening.
The "Little or No Loss" results for both ears are shown in the screen capture. This level of hearing is typical for healthy individuals under 30 if lifetime noise exposure has been low. Healthy teenagers may show hearing levels up to -10 dB (the lower the better).
This puts my hearing in the 90th to 95th percentile for people in my age group (70+), despite a lifetime of listening to loud music starting with the Beatles, Rolling Stones, and Pink Floyd in the late 1960s.
In some cases, supplementation with B-12 (especially methylcobalamin) has been associated with partial improvement in hearing thresholds or tinnitus when addressed early. Though not a primary treatment for hearing disorders, B-12 plays a supportive role in preserving auditory nerve function, and its deficiency should always be ruled out in unexplained or progressive hearing loss.
Eyesight loss protection. B-12 is critical for the health of the optic nerve, and deficiency can lead to a condition known as optic neuropathy. It results in blurred vision, reduced color sensitivity, or central visual field defects, typically in both eyes. The damage is often misattributed to aging, glaucoma, or other causes, but sometimes it is reversible with early B-12 supplementation.
In severe cases, long-standing B-12 deficiency can lead to permanent vision loss from nerve atrophy. Smokers and heavy drinkers with poor diets or malabsorption issues are at the highest risk.
Although B-12 is not a vision-enhancing supplement in the conventional sense, it is essential for maintaining optic nerve integrity and preventing neurologically mediated vision loss. It should be considered in any case of unexplained visual decline, especially if accompanied by other neurological symptoms.
My wife Tatyana, who is also 70 and takes the same supplements, can still read the proverbial 'small print' (less than 6 points) without eyeglasses in average lighting. People often find this shocking, and some even accused her of wearing contacts and lying. More about Tatyana is here: Why having good luck and good genes isn't enough?
Libido and fertility protection. B-12's role in supporting libido is indirect but significant. By maintaining healthy nerve conduction and neurotransmitter balance, B-12 helps sustain the neurological conditions required for sexual interest and responsiveness.
Since B-12 is essential for red blood cell production and oxygen transport, poor oxygenation can impair arousal in both sexes and contribute to erectile difficulties in men. These effects are often misattributed to stress, aging, or relationship issues when the real cause is physiological.
Since libido is closely tied to good mood and energy, the chronic fatigue and low mood that often accompany B-12 deficiency can significantly reduce sexual motivation in both men and women.
In terms of fertility, B-12 plays a more direct role. In women, it supports folate metabolism and methylation, both of which are critical for egg quality, ovulation, and implantation. Low B-12 levels have been associated with increased miscarriage risk and may disrupt hormone balance by impairing estrogen and progesterone clearance. In men, B-12 supplementation has been shown to improve sperm count, motility, and DNA integrity, especially in cases of idiopathic (cause unknown) infertility.
-
Appetite and growth in infants and children.Vitamin B-12 plays a central role in early brain development, appetite regulation, and the maturation of the nervous system. During infancy and early childhood, the demand for B-12 is especially high because of rapid brain growth and the formation of neural connections that lay the foundation for cognitive, motor, and emotional function. Deficiency during this period can lead to failure to thrive, developmental delays, poor feeding, low muscle tone, and long-term cognitive impairment.
Breast milk or infant formula is the sole source of B-12 in the first year of life since infants cannot chew or digest animal products and do not yet produce enough stomach acid or intrinsic factor to extract and absorb B-12 from solid foods.
For these reasons, infants are entirely dependent on the mother's B-12 status or the adequacy of formula fortification to meet their needs. If a breastfeeding mother is deficient, the infant may develop symptoms within months, and the neurological damage can become irreversible if not promptly identified and corrected.
I believe vitamin B-12 deficiency is one of the drivers of the autism epidemics in the United States over the past two generations because of the radical changes and attitudes toward red meat and organ foods among all social classes, on the one hand, and extensive anti-supplementation propaganda by the medical establishment on the other.
Beyond the cardiovascular system, high homocysteine levels are associated with cognitive decline, memory loss, and depression, especially in older adults. It is considered a risk factor for Alzheimer’s disease and vascular dementia, not because it causes these conditions directly, but because it contributes to the long-term damage that leads there.
Vitamin B-12 helps keep homocysteine in check. If B-12 is low, even a healthy diet won't be enough to keep levels stable. That’s why maintaining adequate B-12 for protecting your heart, brain, and blood vessels.
Optimal dosing ranges and rationale for 1,000 mcg
The recommended dietary allowance (RDA) for vitamin B-12 in healthy adults is absurdly low, just 2.4 mcg per day. It was based on research from late 1990s, focusing on preventing deficiency rather than providing an optimal amount. That number also assumes perfect absorption and full digestive capacity, which rarely applies in real life. In practice, only 1% to 2% of an oral B-12 dose is passively absorbed without intrinsic factor, which is why higher doses are necessary to overcome poor assimilation.
A sublingual dose at 1,000 mcg sidesteps these limitations. It ensures that enough B-12 reaches the bloodstream through the oral mucosa, even in people with low stomach acid, damaged gut lining, or intrinsic factor deficiency. This dose has been shown to restore B-12 levels as effectively as injections, particularly when used consistently.
Clinical studies and real-world protocols commonly use 1,000 mcg to 5,000 mcg per day for deficiency correction, with lower maintenance doses afterward. Our 1,000 mcg sublingual formula strikes a balance: it delivers a therapeutically active dose without overwhelming absorption capacity or causing waste, and it is safe for long-term, daily use.
In cases of diagnosed deficiency or high metabolic demand, multiple doses per day may be appropriate under guidance, but for general support, 1,000 mcg daily is a well-established and effective standard.
Risks of over-supplementation or long-term use
Vitamin B-12 is water-soluble, and excess amounts are generally excreted in urine. Unlike fat-soluble vitamins, it does not accumulate to toxic levels. Decades of clinical use, including injections, sublingual tablets, and high-dose oral therapy, have shown no established upper limit for safety, even at doses exceeding 5,000 mcg per day.
Methylcobalamin used in our formula appears far less likely to cause any side effects than synthetic cyanocobalamin, particularly when taken in physiologic doses such as 1,000 mcg per day.
For long-term users, the main concern is not toxicity but masking of folate deficiency or misinterpretation of lab results. When used in isolation without checking other B-vitamin status, B-12 can correct pernicious (i.e., injurious, destructive) anemia while allowing underlying imbalances to persist.
In summary, daily sublingual B-12 at 1,000 mcg is safe, well-tolerated, and appropriate for long-term use, especially in individuals with chronic low intake, impaired absorption, or ongoing metabolic demand. No on/off cycling or "detox periods" are required.
How to take
Dissolve one tablet under the tongue once daily or as needed. Do not chew or swallow. Allow it to dissolve to ensure maximum absorption through the oral mucosa. For individuals with known deficiency, poor absorption, or high metabolic demand, the dose may be repeated once more later in the day. No water or food is required before or after use. Safe for long-term daily use.
Do not take B-12 the day before and on the day of a blood test because it will temporarily elevate blood levels and distort results. If your doctor flags “excessively high” B-12 on your lab report, let them know that you are taking a sublingual formula. High levels after supplementation are expected and not harmful. Most lab ranges are designed for detecting deficiency, not assessing optimal or functional levels during supplementation.
Storage and stability
Store in a cool, dry place away from direct sunlight, heat, and humidity. Do not refrigerate. Keep the bottle tightly closed between uses to prevent moisture exposure, which may cause the tablets to soften or degrade. Our coenzymated B-12 is stabilized without synthetic preservatives, so proper storage is essential to maintain potency. When stored correctly, the product remains effective through its expiration date printed on the label.
Special cases
GLP-1-assisted Weight Loss. All Ozempic-class medications slow gastric emptying, reduce stomach acid, suppress appetite, and lead to prolonged periods of low protein intake. These changes disrupt every step required to absorb B-12 from food: protein digestion, acid release, intrinsic factor production, and ileal transport. Over time, this puts users at high risk of B-12 depletion, even with a seemingly adequate diet. Sublingual B-12 bypasses the compromised digestive route entirely and is the most reliable delivery method under these conditions.
To prevent fatigue, nerve damage, and cognitive decline caused by impaired B-12 absorption during weight loss therapy, begin supplementation at the start of GLP-1 therapy, not after symptoms emerge. Waiting until blood levels drop or neurological signs appear can result in permanent deficits. Continue supplementation for as long as GLP-1 therapy is ongoing and for up to 6 months afterward, during the tapering or recovery period.
Long-Term Fasting or Caloric Restriction. Extended and intermittent fasting and very low-calorie diets fail to provide enough B-12 over time. These regimens may also suppress stomach acid production, further reducing the body’s ability to extract B-12 from food. Sublingual B-12 is a safe, non-caloric tool for preventing depletion during prolonged dietary restriction.
High-Stress Occupations. Chronic psychological or physical stress increases the body’s need for methylation, neurotransmitter synthesis, and adrenal support, which depend on adequate B-12. Individuals in demanding jobs often experience fatigue, sleep disruption, and mood instability that mimic early B-12 deficiency, even if blood levels are technically within range. Regular use of sublingual B-12 can help support mental clarity, energy, and recovery capacity under sustained stress conditions, particularly when paired with irregular meals or low-protein intake.
Vegan and Vegetarian Diets. Vitamin B-12 is found only in animal-derived foods. Plant-based diets, including vegan and most vegetarian patterns, lack a reliable source unless fortified foods or supplements are used consistently. Even mild deficiency can develop after 1–3 years, often without warning signs. Supplementation is essential to prevent fatigue, neurological symptoms, and long-term cognitive or developmental deficits. Sublingual forms are preferred for steady maintenance, especially in individuals with low total protein intake or irregular eating patterns.
Adults Over 40. The stomach acid production declines with aging, a condition known as hypochlorhydria. Acid deficiency makes it harder to release B-12 from food proteins. Even with a balanced diet, absorption becomes less efficient, especially in those with atrophic gastritis or frequent use of acid-suppressing medications. Up to one-third of adults over 65 have subclinical or overt (obvious) B-12 deficiency, often misattributed to aging itself. Supplementation with a sublingual form bypasses gastric limitations and helps maintain energy, cognitive clarity, and neurological stability. If you'd rather not deal with the mental decline of your parents or partners, recommend they take B-12 daily.
Long-Term Use of Acid-Suppressing Drugs (PPIs, H2 Blockers). Proton pump inhibitors (like omeprazole and lansoprazole) and H2 blockers (like famotidine and ranitidine) reduce stomach acid production. This impairs the release of B-12 from food, leading to gradual depletion even with adequate intake. Long-term users, especially those taking these drugs daily for GERD, ulcers, or gastritis, are at elevated risk of sublcinical (silent) deficiency. Sublingual B-12 bypasses the need for gastric acid and is the preferred route for maintaining normal levels.
Metformin Users. Metformin, commonly prescribed for type 2 diabetes and PCOS, interferes with B-12 absorption. The risk of deficiency increases with the dose and duration of therapy and often goes unnoticed until symptoms such as fatigue, neuropathy, or anemia appear. Regular supplementation with sublingual B-12 is a simple preventive measure for anyone using metformin daily.
Bariatric Surgery Patients. Procedures like gastric bypass and sleeve gastrectomy permanently alter or remove the parts of the stomach and small intestine responsible for B-12 release, intrinsic factor secretion, and absorption. Without supplementation, deficiency is inevitable and can appear within months. Sublingual B-12 is the standard of care for long-term maintenance and should be taken for life unless managed with regular injections.
Chronic Alcohol Use. Alcohol damages the stomach lining, reduces nutrient absorption, and depletes liver stores of B-12 over time. It also interferes with the conversion of B-12 into its active forms. Even moderate but sustained alcohol intake can contribute to deficiency, especially when paired with a poor diet. Supplementation with an active, sublingual B-12 helps restore levels without relying on impaired digestive function.
Pernicious Anemia and Autoimmune Gastritis. These conditions destroy the stomach cells that produce intrinsic factor, making it impossible to absorb B-12 through food or standard oral supplements. Without treatment, irreversible neurological damage may occur. Sublingual B-12 is often sufficient to bypass this defect, offering a non-invasive alternative to injections for long-term management.
Chronic GI Conditions.Diseases such as Crohn’s, celiac, and small intestinal bacterial overgrowth (SIBO) can interfere with B-12 absorption by damaging the intestinal lining or altering normal digestive function. Even during remission, patients may absorb only a fraction of dietary B-12. Sublingual supplementation provides a direct and reliable method of correction without adding digestive strain.
Pregnancy and Lactation. B-12 demand increases during pregnancy to support fetal brain and nervous system development and remains elevated during breastfeeding. Infants receive B-12 exclusively through the mother’s milk, placing mothers with low intake or absorption at high risk of depleting both themselves and the child. Sublingual B-12 is well-tolerated and provides consistent delivery without relying on digestive variables that may fluctuate before, during, and after pregnancy.
Chemotherapy and Radiation Therapy.Both chemotherapy and radiation damage rapidly dividing cells, including those in the bone marrow and digestive tract. This increases the body’s demand for B-12 while simultaneously impairing absorption and storage. B-12 is also essential for tissue repair, DNA synthesis, and neurological recovery, all of which are stressed during and after treatment. Sublingual B-12 helps support recovery by bypassing the damaged digestive system and ensuring reliable delivery to metabolically active tissues.
Before and After a Major Surgery.Surgery places a sudden demand on the body’s repair systems, immune response, and red blood cell production, all of which require B-12. Anesthesia, fasting, blood loss, and medication can further deplete reserves or disrupt absorption. Taking B-12 before surgery improves resilience and postoperative recovery. Supplementation should continue for several weeks after surgery, especially if food intake or digestive function is impaired. Sublingual B-12 provides a simple and effective way to maintain optimal levels during this critical window.
Convalescence from Major Trauma or Illness.Recovery from serious illness, injury, or prolonged hospitalization places intense demands on the body’s healing systems. Protein metabolism, red blood cell production, neurological repair, and immune function all rely on sufficient B-12. At the same time, appetite is often reduced and digestive function compromised. Sublingual B-12 supports recovery by providing a direct route to replenish what’s lost without depending on food intake or intestinal absorption.
Long COVID. Post-viral syndromes are marked by fatigue, brain fog, nerve dysfunction, and inflammatory stress, symptoms that overlap significantly with B-12 deficiency. While B-12 is not a treatment for Long COVID itself, many patients experience improvement when subclinical deficiencies are corrected. The neurological and mitochondrial support provided by methylcobalamin makes it a relevant adjunct for recovery, especially in individuals with poor intake or previous GI disorders.
Lyme Disease (and Post-Treatment Recovery). Lyme disease and its treatment can leave lasting effects on the nervous system, energy metabolism, and cognitive function. Chronic inflammation, immune stress, and medication side effects may reduce B-12 absorption or increase demand. B-12 is particularly useful during the recovery phase when fatigue and neuropathic symptoms persist. Sublingual administration helps bypass any gastrointestinal disruption and ensures steady delivery to tissues under repair.
All the conditions I’ve described above are just the tip of the iceberg. If you’re wondering why governments don’t recommend universal B-12 supplementation or why the official daily value is still stuck at 2.4 mcg, the answer is as simple as it is cynical: the longer you live in good health, the more they have to spend on your pensions, medical insurance, and long-term care. That’s not a financial model anyone in charge wants to encourage.
Frequently Asked Questions 
Q. My B-12 blood level is high, but I still have deficiency symptoms. How is that possible?+
Most standard blood tests measure total circulating B-12, including inactive forms such as cyanocobalamin or hydroxycobalamin found in low-cost supplements that you may be taking. In such cases, high levels may simply reflect what you took, but not actual cellular uptake.
Mutations in the MTHFR or MTRR genes and liver dysfunction are common causes of impaired conversion of cyanocobalamin or hydroxycobalamin into methylcobalamin (the active form). Switching to sublingual or injected methylcobalamin bypasses this step and may resolve your deficiency symptoms.
Q. How do I know if I need to take B-12?+
If you're dealing with low energy, memory lapses, numbness, tingling, burning sensations, poor concentration, mood swings, swollen tongue, mouth sores, or following a restricted diet, B-12 is one of the first things to consider. These symptoms are common even when blood work looks normal. Deficiency is often missed until it’s advanced. If any of the conditions discussed above apply to you, don’t wait for a formal diagnosis. B-12 is safe, inexpensive, and often improves symptoms within weeks if it’s part of the problem.
Q. Can I take B-12 without a blood test?+
Yes, you can. B-12 is one of the few supplements that is safe to take preventively, even without lab confirmation. Blood tests can be misleading, especially if you’ve supplemented recently or have liver or kidney conditions that distort serum levels. If you’re in any of the risk groups mentioned above or already experiencing relevant symptoms, it makes more sense to start supplementation than to wait for a test to catch up with reality.
Q. How long do I need to take it?+
It depends on your situation. If you’re taking B-12 for prevention because you’re older, on a restricted diet, or taking medications that interfere with absorption, then you’ll likely need to take it indefinitely.
If you're planning to get pregnant, you and your husband should start taking B-12 at least 6 months before conception, continue through the entire pregnancy, lactation, and for another 6 months afterward to recover, or expect to deal with postpartum depression, compromised breastfeeding, a poorly developed child, and a potentially ruined marriage.
After age 40, I’d recommend taking it for life. The same goes for vegans and vegetarians at any age. I've been taking sublingual B-12 every day since 1996. That’s one of the reasons I’m still more or less intact, unlike 95% of men in my age group. Ditto my wife and extended family. More details here: Why Should You Trust Me?
Q. Can I take too much? Is 1,000 mcg safe?+
Yes, it’s safe. B-12 is water-soluble and doesn’t accumulate to toxic levels. What your body doesn’t use is simply excreted in the urine. Clinical trials have used daily doses far higher than 1,000 mcg without adverse effects. In fact, 1,000 mcg is the minimum dose often needed to bypass absorption problems and restore normal function. Unless you have a rare medical condition that alters B-12 handling, there’s no downside to this dosage.
You’ve probably heard the tired line that supplements just “make expensive urine.” If someone says that to you, remind them that a part of everything we consume — food, water, and medication — leaves the body exactly the same way. And while you’re at it, ask that naysayer to put you on their will so that you can take care of their children and pets after their "cheap urine" stops flowing.
Q. Can I use B-12 during pregnancy or breastfeeding?+
Absolutely. B-12 is critical during both. The developing fetal brain depends on it, and so does the production of breast milk. So does your postpartum recovery.Deficiency in the mother can lead to long-term neurological damage in the child. It’s often missed during pregnancy because doctors don’t routinely test for it. The safest option is to supplement early and consistently. The dose in this product is appropriate for daily use during all stages of pregnancy and nursing.
Q. Is this formula suitable for vegans and vegetarians?+
Yes. The active ingredient in this formula is synthesized without animal products and is suitable for vegans and vegetarians. There are no hidden gelatin, dairy, or animal enzymes in this formula.
Q. Can I take this with other supplements or medications?+
Yes, you can unless your doctor instructs you otherwise and tells you why. B-12 doesn’t interfere with most medications or supplements. It’s often taken alongside folate, iron, or B-complex vitamins. There are no known negative interactions with drugs that would require avoiding this supplement, though some medications may reduce B-12 absorption. That’s exactly why you should be taking it in sublingual form.
Q. I don’t want to take synthetic drugs. Can I get a natural formula for B-12?+
If by “natural” you mean B-12 that comes directly from food, the answer is no, because there is no reliable food-based B-12 supplement on the market.
All supplemental B-12, including ours, is synthesized by bacterial fermentation in a lab environment. The body doesn’t care whether B-12 came from a steak, a capsule, or a fermentation tank. It only cares whether it’s in a usable form and still bioactive. In that sense, our formula is biologically “natural,” even though it's not extracted from food.
If you’re looking for something truly food-based, your only options are animal liver, rare steak, or shellfish, neither of which are viable for people with absorption issues or dietary restrictions.
Q. Can I take this formula with Once Daily Multi, which also contains 250 mcg of B-12?+
Yes. Oral B-12 formulas have lesser absorption because they depend on the intrinsic factor and a perfectly healthy stomach and intestines. The sublingual formula delivers B-12 directly into the bloodstream, bypassing the digestive system altogether. Taking both is not harmful.
Q. I see on Amazon a similar B-12 for half the price. Should I take them?+
Most of the B-12 supplements sold on Amazon are manufactured in China or made from consumer-grade components under Chinese quality standards. That’s why they’re cheaper. In contrast, professional-grade formulas like ours or from top-tier vendors like Douglas Labs, Pure Encapsulations, and Thorne typically retail for $20 to $25.
Also, our supplements are produced in small batches, which means they are fresher. That matters because coenzymated formulas like B-12 are fragile and degrade over time, particularly when stored in warehouses for longer periods of time.
Author’s Note
Back in medical school in the early 1970s, one of our professors casually mentioned that older members of the ruling elite routinely received weekly intramuscular vitamin B-12 injections to keep their minds sharp and their bodies going well into old age. That offhand remark stuck with me. If those 'old farts' were staying functional into their seventies and eighties, why wouldn’t I take one tablet a day for the rest of my life?
Looking back, taking B-12 daily since my early forties, along with other essential supplements, was one of the best decisions I’ve ever made.I did it because I couldn’t afford to slow down, and I understood early on that once the nervous system goes, it doesn’t come back.
I’m still wearing eyeglasses and have been since I was three, but I don’t have cataracts or macular degeneration. I am free of chronic fatigue, no early dementia, no mystery pain, no prescriptions. I can write for 16 hours straight (with small breaks, of course), read dense material in three languages without losing focus, and walk for miles without stiffness or soreness.
For more context on why I take B-12 daily and how that fits into the broader picture of staying functional into my early seventies. You can read my note here: Why Should You Trust Me?
Further Reading and References
The following sources provide additional background on the clinical significance, dietary considerations, and systemic functions of vitamin B-12. They include institutional fact sheets, peer-reviewed reviews, and large-scale nutritional surveys that you may want to explore in greater depth.
NIH Office of Dietary Supplements – Vitamin B12 Fact Sheet
https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/
Linus Pauling Institute – Micronutrient Information Center: Vitamin B12
https://lpi.oregonstate.edu/mic/vitamins/vitamin-B12
Cleveland Clinic – Vitamin B12 Deficiency
https://my.clevelandclinic.org/health/diseases/22831-vitamin-b12-deficiency
National Institutes of Health – Vitamin B12 and Health (PubMed)
Green R, et al. Vitamin B12 deficiency. Nat Rev Dis Primers. 2017;3:17040.
https://www.nature.com/articles/nrdp201740
British Journal of Nutrition – Global Prevalence of Vitamin B-12 Deficiency
Allen LH. Causes of vitamin B12 and folate deficiency. Food Nutr Bull. 2008;29(2 Suppl):S20–S34.
https://pubmed.ncbi.nlm.nih.gov/18709879
Merck Manual – Vitamin B12 Deficiency
https://www.merckmanuals.com/professional/nutritional-disorders/vitamin-deficiency-dependency-and-toxicity/vitamin-b12-deficiency
American Journal of Clinical Nutrition – Vitamin B-12 concentration and memory performance in patients with mild cognitive impairment
Smith AD, Refsum H. Homocysteine, B Vitamins, and Cognitive Impairment. Volume 103, Issue 4p1045-1054April 2016
https://ajcn.nutrition.org/article/S0002-9165(23)11928-9/
USDA FoodData Central – B-12 Content in Foods (manual search)
https://fdc.nal.usda.gov/
The Food and Drug Administration has not evaluated this information. This product is not intended to diagnose, treat, cure, or prevent any disease.