
How to Self-Diagnose Mineral Deficiencies
Until very recently, the quality of one’s life was determined by the good fortune of being born in the right place to the right parents. The luckiest of all were people born in the mountainous regions of Europe, Central Asia, Japan, and South America.
These regions offered pristine, mineral-rich water flowing from natural springs, untouched by modern processing and filtration. The same water nourished the soil, plants, and livestock, creating a complete food chain naturally enriched with essential macro- and trace elements.
People raised on this land enjoyed robust physical development, low rates of chronic disease, and some of the longest, healthiest lives recorded in modern history. The better-known regions with mineral-rich water and long-lived populations include:
-
The Swiss and Austrian Alps are historically associated with sturdy health, low rates of chronic disease, and clean mountain agriculture. Roman popes traditionally recruited their Swiss Guards from this region because these men were visibly larger, healthier, and fitter than the average Roman.
-
The Caucasus Mountains (Georgia, Armenia, Azerbaijan) are renowned for exceptional longevity and abundant mineral springs that supply water and irrigate crops and pastures.
-
Sardinia is a blessed Italian island with access to mineral-rich spring water and a traditional diet based on local produce and animal foods.
-
Andean Highlands (Peru, Ecuador, Bolivia) are known for nutrient-dense soils, glacial runoff, and traditional diets built around native grains and pasture-raised livestock.
-
Japanese Alps and Okinawa are regions where natural spring water and mineral-rich sea-derived foods have supported healthy aging and physical vitality for generations.
All these longevity clusters share common environmental factors: high mineral content in water and soil and traditional lifestyles that preserved the nutritional integrity of food and water sources.
Today, you can recreate the most critical parts of those ideal conditions for yourself and your children with professiona-grade supplements from this site or similar from Douglas Labs or Pure Encapsulation, San Pellegrino mineral water from Costco, and New Zealand's lamb from Whole Foods.
That would be your best defense from not ending up prematurely aged and overmedicated like the majority of middle-aged urban American men and women.
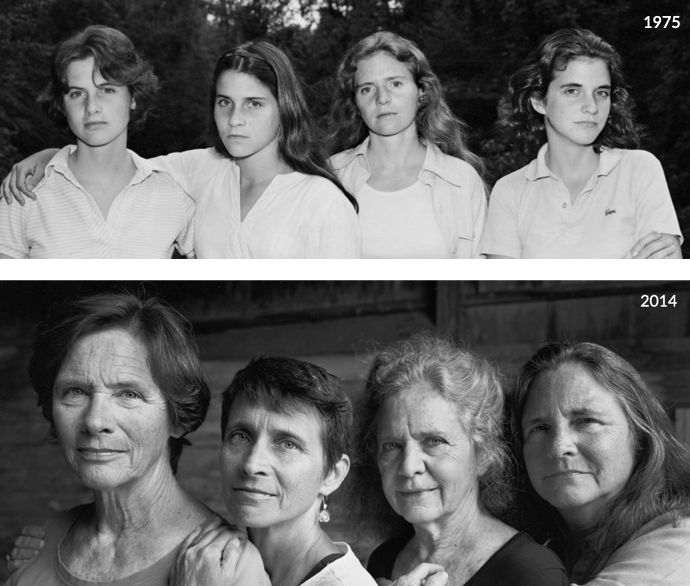
To illustrate what I mean, take a look at these two sets of photos from the famous Brown sisters' photo series that I analyzed on the Why You Should Trust Me page:
The Extraordinary Portraits of the Brown Sisters
by Google Arts and Culture [link]
Shown above, from the left are Heather (23), Mimi (15), Bebe (25), and Laurie (21) in 1975, and below in 2014. They were photographed each year between 1975 and 2014 by the husband of Bebe, a renowned American photographer, Nicholas Nixon.
Looking at these photos, it's truly striking how these four attractive American women from apparently a well-to-do background had aged beyond recognition, as if their lives were spent in profound Dickensian poverty and hard labor.
Here are, for comparison, three candid unretouched photos of my wife Tatyana, who was born in January 1955, so she and Laurie Brown (first from the right in the photos above) are the same age, except that Tatyana in these photos is nine years older:

What gives? Was Tatyana born, raised, and lived in the French Alps or Sardinia? No, she wasn't. Is she idle-rich? No, she isn't. She started working full-time right after high school and is still working. Did she take Ozempic or have plastic surgery? No, she hadn't. Was she a gym junkike? Never set a foot.
The only difference between Tatyana and the Brown sisters is that she is my wife, so her nutrition and supplementation from 1996 on was the same as mine, plus/minus more permissive for fruits and desserts, because, unlike me, she hasn't been affected in the past by type 2 diabetes.
The rest of this page is focused on describing the role of minerals in health and nutrition, and how to identify nutritional disorders related to their deficiencies.
Systemic Symptoms of Mineral Deficiencies
Dietary minerals are classified into two main categories based on their quantities in the body:
Macrominerals are required in gram-level amounts and include calcium, magnesium, potassium, sodium, chloride, phosphorus, and sulfur. In this article and similar texts, the term “minerals” typically refers to this group.
Trace elements, also called microelements, are needed in much smaller amounts but are just as essential. They include iron, zinc, copper, iodine, selenium, chromium, manganese, and molybdenum. (I'll provide a full breakdown of trace elements in Part III of this cycle.)
The widely used term electrolytes refers to the charged ions of sodium, potassium, chloride, calcium, and magnesium. These ions help regulate the body’s fluid volume, composition, and distribution across cells, tissues, and blood plasma.
Unlike well-known minerals like calcium, magnesium, potassium, zinc, and chromium, trace elements other than iron, zinc, and chromium are seldom discussed, and their deficiencies are rarely recognized for several interconnected reasons:
Many of these micronutrients are required in extremely small amounts. Deficiency signs are often subtle, nonspecific, or overlap with more familiar nutrient imbalances, making clinical recognition difficult.
Their effects tend to manifest gradually or in combination with other deficiencies, complicating diagnosis.
Medical education, public health messaging, and nutritional guidelines emphasize the "major" minerals because they are linked to well-defined deficiency syndromes and are easier to study and measure.
Health professionals, policymakers, and supplement manufacturers focus on minerals involved in bone health, electrolyte balance, and immune support because they are easier to explain and market to the public.
Deficiency symptoms for many trace elements resemble common chronic conditions and often go unnoticed until advanced stages. Without specific testing, they are unlikely to be identified.
Clinical syndromes typically occur only under extreme conditions such as severe malnutrition, rare genetic disorders, or prolonged medical restrictions. Routine screening is rare unless a physician suspects it, which is uncommon outside of fictional cases like Dr. House.
Trace elements are difficult to assess due to their low concentrations, inconsistent bioavailability, nutrient interactions, and individual health variables. Most physicians lack training in this area, and qualified specialists are scarce.
There are two notable exceptions in the case of iodine and fluoride.
Iodine deficiency is taken seriously in the United States, largely because of the long-standing practice of iodizing salt. This iodization has dramatically reduced the incidence of goiter and cretinism, which were common in the early 20th century.
However, at the same time, an overwhelming anti-salt message has permeated media, health campaigns, and public discourse, warning consumers about high sodium intake and its relationship to hypertension and cardiovascular disease.
As a result, many people reduce salt consumption without realizing that this also limits the intake of iodine. Without enough iodine, especially during pregnancy and early childhood, a child’s brain development and thinking abilities can suffer.
I believe iodine deficiency may be one of the primary factors behind a crazy-high increase in autism. Its rate in the United States between the 1950s and 1960s ranged from 0.5 to 4 cases per 10,000 children. By 2025, it has risen to 1 in 36 children. Depending on the initial baseline, this sad statistic represents an approximately 70- to 600-fold increase over just four generations.
Fluoride deficiency is a more complex story because it increases the risk of dental caries, while overexposure may impair bone health and exacerbate trace element imbalances. It is a trace element found naturally in water, soil, and some foods, and is best known for its use in toothpaste and water fluoridation to prevent cavities.
Excess fluoride exposure can result in dental fluorosis (enamel mottling) or skeletal fluorosis (bone changes), most notably in children and in regions with naturally high levels.
High intake of fluoride can also interfere with calcium and magnesium metabolism, especially among people with already inadequate intake. For these reasons, fluoride isn't considered essential for systemic health beyond its effects on teeth.
Some water treatment processes that add fluoride may also remove other beneficial minerals and trace elements during filtration, which may contribute to broader population-level deficiencies.
The trace elements strontium, vanadium, nickel, silicon, fluoride, lithium, and arsenic are present in the body in very small amounts but are not universally recognized as essential for human health. They are excluded from this article because there are no standardized intake recommendations, and their therapeutic use remains experimental or controversial.
With all the theory behind us, let’s get to the meat and potatoes of this article. The following summary outlines the primary disorders caused by mineral and trace element deficiencies. Some conditions may be linked to more than one mineral or trace element.
Calcium Deficiency
Calcium (Ca) is an essential macromineral and electrolyte. The body contains approximately 1,200 grams of calcium. The 99% stored in bones and teeth, and the remaining 1% found in blood, muscles, and intracellular fluid. It plays a central role in maintaining skeletal structure, supports muscle contraction, nerve transmission, blood clotting, and the regulation of hormones, enzymes, and metabolic processes.
Bones serve as the primary storage site for calcium, phosphorus, and smaller amounts of magnesium, sodium, and trace elements. When the diet doesn't provide enough minerals, the body draws on these reserves to maintain stable blood levels (homeostasis) and support metabolic processes.
The process of releasing calcium and phosphorus into the bloodstream is carried out by osteoclasts and is called resorption. Osteoblasts perform the reverse function by depositing calcium back into the bones.
Dietary Sources of Calcium
Calcium is obtained from drinking and cooking water, and food such as milk, cheese, yogurt, bone broth, leafy green vegetables (collard greens, kale, bok choy), fortified foods (orange juice, plant milks, cereals), nuts, and small fish with bones (such as sardines).
When calcium intake is inadequate or intestinal absorption is impaired, the continuous resorption leads to osteopenia (early-stage bone loss), osteoporosis (brittle bones), and osteomalacia (soft bones).
The “eight glasses of water a day” dogma, heavily promoted in the United States by the bottled water industry, accelerates these conditions in both young and old because excess water leaches calcium from bones like no other factor. It is also a major contributor to kidney stones. I describe this paradox in depth in the Water Damage chapter of Fiber Menace.
Below is a breakdown of primary health conditions linked to calcium deficiency, and organized by affected organs or systems:
Skeletal Disorders
Osteopenia and Osteoporosis. Chronic deficiency leads to a gradual loss of bone mineral density, predisposing both women and men (especially postmenopausal women and older adults) to osteopenia (mild bone loss) and osteoporosis (severe bone fragility and increased fracture risk).
Rickets. In growing children, calcium deficiency (often in combination with vitamin D deficiency) can result in rickets, marked by bone deformities and impaired growth.
Osteomalacia. In adults, insufficient calcium can cause osteomalacia, characterized by soft and weak bones, bone pain, and muscle weakness.
Neuromuscular Disorders
Muscle Cramps and Spasms. Early signs of deficiency include muscle cramps, spasms, and tingling sensations, particularly in the hands, feet, and around the mouth.
Tetany. Severe deficiency may provoke tetany—a state of involuntary muscle contractions and twitching, tremors, and in extreme cases, seizures.
Cardiovascular and Other Systemic Effects
Abnormal Heart Rhythm. Low blood calcium can affect the electrical signaling of the heart, leading to arrhythmias and, in some cases, cardiac arrest.
Numbness and Paresthesia. Sensations of numbness or “pins and needles” may occur as calcium-dependent nerve conduction becomes impaired.
Impaired Blood Clotting. Calcium is needed for proper blood coagulation, and deficiency can exacerbate bleeding or delay blood clotting.
Dental Disorders
Tooth Decay. Insufficient calcium during periods of tooth formation (childhood, adolescence) increases the risk for delayed dental development, defective enamel, and increased cavity risk.
Periodontal disease. Calcium deficiency weakens alveolar bone and impairs tooth anchoring, increasing the risk of gingival inflammation, tooth mobility, and eventual tooth loss.
Jaw bone development. Calcium deficiency during childhood and adolescence impairs jawbone development. When the maxilla and mandible do not grow to their full genetic potential, tooth crowding and misalignment lead to lifelong dental problems.
Growth and Developmental Disorders
Calcium and vitamin D are essential for bone growth and mineralization during childhood and adolescence. When calcium intake is inadequate, growth plates (epiphyseal plates) may not ossify properly, leading to delayed skeletal development. Here are all of the associated disorders:
Delayed skeletal maturation. Inadequate calcium disrupts ossification and delays growth plate closure, impairing normal bone development.
Rickets (with vitamin D deficiency). Leads to bone softening, skeletal deformities, bowed legs, and delayed dentition.
Scoliosis. Weak and under-mineralized vertebrae may fail to support proper spinal alignment during growth spurts, increasing the risk of lateral spinal curvature.
Delayed motor development. Poor bone strength and muscle function can slow the acquisition of gross motor milestones.
Dental abnormalities. Defective enamel formation and delayed tooth eruption raise the risk of decay and malocclusion.
Increased fracture risk. Low bone density heightens susceptibility to fractures even from minor trauma.
Potential cognitive or behavioral effects. Chronic calcium deficiency, especially when compounded by other micronutrient deficits, may impair overall neurological development.
Medications and OTC Drugs That Contribute to Calcium Deficiency
Proton pump inhibitors (PPIs) (omeprazole, lansoprazole) suppress stomach acid, reducing the solubility and absorption of calcium carbonate.
H2 receptor antagonists (ranitidine, famotidine). Reduce gastric acid secretion, similarly impairing calcium absorption.
Statins (e.g., atorvastatin, simvastatin, rosuvastatin) inhibit endogenous cholesterol synthesis, which reduces the substrate (7-dehydrocholesterol) required for vitamin D3 production in the skin. Lower vitamin D levels impair calcium absorption in the intestines and increase the risk of calcium deficiency over time.
Corticosteroids (prednisone, dexamethasone) inhibit calcium absorption in the gut, increase renal calcium loss, and suppress bone formation.
Loop diuretics (furosemide, bumetanide) promote calcium excretion through the kidneys, lowering serum levels.
Thiazide diuretics (hydrochlorothiazide) reduce urinary calcium loss. Long-term use may disturb overall calcium balance and vitamin D metabolism.
Anticonvulsants (phenytoin, phenobarbital, carbamazepine). Accelerate vitamin D catabolism, indirectly reducing calcium absorption.
Thyroid hormone replacement (levothyroxine) increases bone turnover and resorption, releasing calcium from bone.
Heparin (long-term use) impairs osteoblast activity and promotes bone resorption.
Aluminum-containing antacids (aluminum hydroxide, found in some OTC indigestion remedies) bind dietary phosphate, leading to compensatory calcium loss from bone via secondary hyperparathyroidism.
Magnesium-based laxatives and antacids (milk of magnesia) interfere with calcium absorption when used chronically.
Fiber laxatives (psyllium) block the absorption of all minerals, not just calcium, in the small intestine.
Caffeine in OTC stimulants or energy supplements increases urinary calcium excretion.
High-dose aspirin or NSAIDs (ibuprofen, naproxen) may impair kidney function over time and compromise calcium homeostasis (sability).
Chemotherapy agents (methotrexate, cyclophosphamide) disrupt bone metabolism and cause rapid calcium loss.
Aromatase inhibitors (anastrozole, letrozole) reduce estrogen levels and accelerate bone resorption and calcium depletion. These drugs are used for the prevention and treatment of estrogen-sensitive breast and ovarian cancers.
Medication-Assisted Weight Loss
Ozempic-class drugs such as semaglutide, liraglutide, and dulaglutide contribute to calcium deficiency through several mechanisms:
Reduced dietary intake. By suppressing appetite, GLP-1s lead to significantly lower intake of calcium from all kinds of foods.
Gastrointestinal side effects cause nausea, vomiting, diarrhea, early satiety, reducing nutrient absorption, and limiting calcium availability.
Weight loss–associated bone loss from rapid or sustained weight loss, especially with muscle mass reduction, is associated with decreased bone mineral density. As bone is resorbed, calcium and bone tissue are lost unless offset by collagen and calcium supplements.
Potential interference with vitamin D absorption. Although not direct, fat-soluble vitamin absorption may be impaired in patients who reduce fat intake significantly or experience malabsorption. Vitamin D is required for calcium assimilation in the small intestine.
Fertility, Pregnancy, Lactation, and Postnatal Recovery
A woman’s body requires significantly more nutrients to support fetal development, maternal health, milk production, and postpartum recovery.
Mineral supplementation in general, and calcium in particular, is a must at least a year prior to pregnancy, during pregnancy, throughout breastfeeding, and for at least a year after completing lactation.
This extended window includes the preconception phase, when nutritional status directly affects fertility, implantation, and early embryonic development; the gestational period, when demand for calcium, iron, iodine, and other micronutrients increases dramatically; the lactation period, when nutrients are continuously transferred into breast milk; and the post-lactation phase, when the body must restore depleted mineral and nutrient reserves.
Failing to meet these sustained demands increases the risk of complications for both mother and child, including low bone density, developmental delays, and long-term health deficits.
Other Risk Factors for Calcium Deficiency
All weight loss diets. Most weight loss plans reduce overall food intake, which often leads to insufficient calcium consumption. Additionally, rapid weight loss increases bone resorption, especially if protein intake is low or if the diet is not supplemented properly.
Low intake of dairy or calcium-rich foods. Dairy products are the most concentrated and bioavailable sources of calcium. Individuals who avoid them without compensating with other rich sources or supplements are at higher risk for deficiency over time.
Lactose intolerance or milk allergy. Individuals with lactose intolerance or milk allergy often avoid dairy, the primary calcium source in most diets. Without deliberate intake of calcium-fortified or alternative sources, they may not meet daily requirements.
Strict vegan diets. Vegans who do not consume enough plant-based calcium sources (e.g., tofu, fortified plant milks, leafy greens) or who consume high-oxalate foods that impair absorption are at elevated risk for calcium deficiency.
Malabsorption syndromes (e.g., celiac disease, Crohn’s). These conditions damage the intestinal lining and impair the absorption of calcium and vitamin D. Chronic inflammation and diarrhea further reduce bioavailability and increase losses.
Vitamin D deficiency. Even with adequate dietary calcium, deficiency in vitamin D leads to poor absorption and lower serum calcium levels, often triggering compensatory bone resorption.
Everyone above 50. Natural aging reduces gastric acid secretion and intestinal absorption efficiency. Combined with increased bone turnover, this raises the daily calcium requirement and risk of deficiency in older adults.
Postmenopausal women. Estrogen helps maintain bone density by limiting bone resorption. After menopause, the drop in estrogen accelerates bone loss, making adequate calcium intake even more critical for skeletal health.
Daily Losses of Calcium
Daily losses of calcium occur via several physiological routes necessary to maintain calcium balance in the body. The primary daily calcium losses include.
Urinary losses. Healthy adults typically lose approximately 100 to 250 mg of calcium per day via urine. The kidneys filter calcium and reabsorb most of it; however, the amount excreted varies with dietary intake, parathyroid hormone activity, vitamin D status, and acid–base balance.
Fecal losses. Calcium losses in feces average about 150 to 250 mg daily. This includes unabsorbed dietary calcium as well as endogenous calcium secreted into the gastrointestinal tract through bile and pancreatic secretions.
Sweat losses. Calcium is lost in sweat in smaller amounts, roughly estimated at 20 to 40 mg per day in sedentary individuals. Higher sweat rates during exercise or in hot climates increase this loss.
Increased excretion requires extra calcium intake with diet or supplements to maintain calcium homeostasis, support bone mineralization, and enable physiological functions such as muscle contraction and nerve signaling.
Calcium Relationship with Vitamins for Optimal Assimilation
The absorption and utilization of calcium in the body depend on adequate vitamin status, particularly fat-soluble and water-soluble vitamins that support calcium metabolism.
Vitamin D is critical for calcium assimilation in the small intestine. Without vitamin D, calcium absorption efficiency declines below 10% to 15% and leads to deficiency regardless of intake. Vitamin D also regulates calcium reabsorption in the kidneys and maintains serum calcium levels critical for physiological functions.
Vitamin K2 works along with vitamin D to optimize calcium metabolism. It activates osteocalcin, a protein required for binding calcium to the bone matrix that is required for mineralization and strength. Vitamin K2 also helps prevent calcium deposition in soft tissues such as arteries, reducing the risk of vascular calcification. Adequate vitamin K status ensures that absorbed calcium is properly directed to bones rather than accumulating undesirably elsewhere.
Vitamin C is required for collagen synthesis. Collagen forms the bone matrix that retains calcium phosphate deposits and ensures bone strength and flexibility. Without a healthy bone matrix, calcium has no place to go, and the bones become brittle and prone to fractures.
Vitamin B6 (pyridoxine) supports calcium metabolism via enzymatic processes related to bone health and calcium regulation.
Prevention and Safety Considerations
The calcium's Recommended Dietary Allowance (RDA) for adults ranges from 1,000 to 1,200 mg per day. Consistent calcium intake is a must for lifelong skeletal integrity and overall health.
In my own and my wife's cases, we are still the same height at 70 as we were at 25. By this time, most men and women in our age group are 1" to 2" inches shorter because demineralized skeletal bones compress as people age.
It's even more in people with osteomalacia because bending of the legs and spine takes away from the height even more. We are that "lucky" not because of our relatively austere diet or high-quality water in Northern New Jersey (it isn't), but because we have both been taking the same supplements since 1996.
In Tatyana's case, calcium supplementation started in earnest when she ran into a huge problem with kidney stones in 1995, the complete opposite of what most doctors recommend even today. I describe this story in greater detail here [link]. I simply went along fearing the same.
If you experience symptoms of calcium deficiency or fall into a higher-risk category, quality supplementation is the most reliable method of protection. I take it myself and recommend my clients to take the Conezymated Once Daily Multi as a foundational supplement.
This formula doesn’t provide the full recommended amounts of calcium and magnesium because including them would require adding three extra capsules.
So if you are past 50, or live in a region with processed or mineral-depleted water, or have been diagnosed with osteopenia or osteoporosis, I recommend adding a Cal-Mag Caps formula to your routine alongside Once Daily Multi.
Please note that I have dedicated an extraordinary amount of space and attention to calcium deficiency. Many of the same principles apply to all other minerals and trace elements. To avoid repetition and maintain clarity, I will omit general considerations already covered in this section.
Magnesium Deficiency
Magnesium (Mg) is an essential macromineral and electrolyte. The adult's body contains up to 25 grams of magnesium. About 60% of it is stored in bones, and the rest is distributed throughout muscles, soft tissues, and extracellular fluid. It acts as a cofactor for over 300 enzymatic reactions critical to protein synthesis, glycolysis, DNA and RNA synthesis, nerve conduction, muscle contraction, and energy production.
Magnesium regulates calcium and potassium transport across cell membranes, supports bone mineralization, and is essential for maintaining cardiovascular rhythm, neuromuscular conduction, and glucose and insulin metabolism. It also acts as a cofactor in hundreds of enzymatic reactions involved in ATP production, protein synthesis, DNA and RNA stability, and the regulation of cellular division and renewal processes.
Dietary Sources of Magnesium
Magnesium is abundant in plant-based foods, particularly nuts (almonds, cashews), seeds (pumpkin, sunflower), legumes (black beans, lentils), whole grains (brown rice, quinoa), and green leafy vegetables (spinach, Swiss chard). It is also present in hard drinking water containing dissolved magnesium salts. Families consuming softened or distilled water may have insufficient intake.
Animal-based sources provide smaller amounts of magnesium. They include fish such as mackerel, salmon, and halibut, as well as dairy, eggs, and organ meats. Lean muscle meats contain relatively little magnesium. As a result, carnivore-style diets, especially limited to muscle meat, may fail to meet daily magnesium requirements and increase the risk of long-term deficiency.
Here’s a list of magnesium-related deficiency conditions, grouped by the organs or systems:
Skeletal Disorders
Bone mineralization. Magnesium is an essential building block of bones, together with calcium and phosphorus. It helps control the size, shape, and stability of hydroxyapatite crystals, the main mineral structure in bone tissue. Without enough magnesium, bones become weaker and more prone to breakdown.
Tooth development. Magnesium supports dentin formation and helps maintain the integrity of alveolar bone, which anchors teeth within the jaw. Deficiency may impair both tooth mineralization and periodontal stability, increasing the risk of early decay and tooth loss.
Bone Mineral Density Reduction. Magnesium deficiency weakens bone structure by impairing osteoblast function, promoting bone resorption, and altering calcium and parathyroid hormone regulation. It works along with calcium and vitamin D, and deficiency in any of the three increases the risk of osteopenia, osteomalacia, and osteoporosis, particularly in postmenopausal women and older adults.
Fracture risk. Low magnesium intake has also been associated with increased fracture risk, even in individuals with otherwise normal calcium intake.
You can see all of the above factors at play in children raised on farms, who display broader facial structures, better-developed jaws, and more robust skeletal builds compared to their urban counterparts from the same ethnic and socioeconomic backgrounds.
These differences are especially noticeable in the alignment of teeth, facial symmetry, height, build, and posture. Farm children typically have greater exposure to mineral-rich well water and whole foods along with meats raised on the same water, while city children are more likely to grow up on soft water and supermarket meats and produce. These are key factors behind divergent patterns in musculoskeletal development.
I’m not suggesting that you need to move your family to a farm. You can achieve many of the same benefits by paying close attention to the quality of the food, water, and supplements you and your children consume each day.
Supplements are particularly important for city dwellers. Over 20 years, their cost is a fraction of what you’re likely to spend on orthodontic treatments and dental care for your children and yourself without supplementation.
When I write this, I can’t escape reminiscing about just how short-sighted, ignorant, and irresponsible most parents are despite all of the resources, education, and access to information available today.
Many obsess over test scores, extracurriculars, and screen time limits, yet pay zero attention to the basic nutritional quality of the food, water, and environment shaping their child’s physical development.
They trust that pediatricians, school lunches, and consumer-grade multivitamins will somehow “cover the bases,” while diet deficiencies quietly take root. By the time dental deformities, poor posture, and behavioral issues emerge, the underlying problems have already compounded, become largely irreversible, and carry an enormous future cost—to both parents and their children.
Neuromuscular Disorders
Fatigue and Weakness. Widespread magnesium deficit contributes to generalized tiredness and muscle weakness.
Muscle Cramps and Spasms. Early deficiency causes muscle cramps, spasms, tremors, and twitching.
Tetany and Seizures. Severe magnesium deficiency may trigger tetany, a term for sustained involuntary muscle contractions, and, rarely, seizures due to neuromuscular hyperexcitability.
Paresthesias. Numbness, tingling, and pins and needles sensations in the feet and hands.
Athletes, outdoor laborers, and older adults are especially at risk for the above conditions because of increased magnesium loss through sweat, reduced dietary intake, and decreased absorption efficiency. These symptoms may intensify during periods of intense exertion, dehydration, or heat exposure, when magnesium-dependent muscle function becomes further compromised.
Cardiovascular Disorders
Arrhythmias and Palpitations. Magnesium plays a critical role in regulating electrical conduction in cardiac muscle. Deficiency can lead to irregular heartbeats, palpitations, and in severe cases, life-threatening arrhythmias such as ventricular tachycardia or fibrillation.
Hypertension. Sustained low magnesium levels are associated with increased vascular resistance and impaired endothelial function, contributing to elevated blood pressure and the progression of atherosclerosis.
Increased Cardiovascular Risk. Chronic magnesium deficiency is linked to increased risk of heart attacks, strokes, and sudden cardiac arrests, particularly in people with metabolic syndrome.
Sudden cardiac arrests of otherwise healthy young athletes have been periodically traced to undiagnosed magnesium deficiency, especially when compounded by fluid loss from sweating and high physical stress.
That's why athletes routinely gulp electrolyte drinks during training or competition: physical exertion, heat, and fluid loss rapidly deplete magnesium, sodium, chloride, and potassium, hurting their performance and putting their heart function at risk.
Metabolic and Endocrine Effects
Glucose Metabolism Impairment. Magnesium is essential for insulin receptor function and glucose transport. Deficiency reduces insulin sensitivity, increases systemic inflammation, and contributes to impaired glucose tolerance, elevating the risk of prediabetes and type 2 diabetes.
Secondary Mineral Imbalances. Low magnesium levels can lead to hypocalcemia and hypokalemia by disrupting parathyroid hormone function and altering renal handling of other electrolytes. These imbalances may cause further neuromuscular and cardiac complications.
Migraines and Headaches. Magnesium deficiency has been linked to increased frequency and severity of migraines. Its role in vascular tone regulation and neurotransmitter balance may explain its influence on migraine threshold and duration. Supplementation has been shown to reduce attack frequency in some individuals.
Dental Health
As I noted previously, magnesium plays a central role in teeth and jaw development, but its impact on oral health extends longer and further.
Increased Risk of Tooth Decay. Magnesium deficiency can reduce enamel hardness and disrupt proper mineralization, making teeth more vulnerable to demineralization and acid erosion from bacterial activity. Both factors increase susceptibility to dental caries.
Gum Disease and Bone Loss. Inadequate magnesium levels are associated with increased systemic and local inflammation, contributing to the onset and severity of periodontitis. Chronic deficiency weakens the alveolar bone around the teeth, potentially worsening tooth mobility and increasing the likelihood of tooth loss.
Psychological and Cognitive Disorders
Mood and Cognitive Disorders. Low magnesium can make people feel irritable, unfocused, mentally tired, and less able to handle stress. These symptoms often creep in gradually and are easy to overlook or misattribute.
Poor Sleep. Magnesium is instrumental in the production of melatonin, a sleep-regulating hormone. When magnesium is low, falling asleep and staying asleep can become harder—especially for older adults, who are already more prone to light or broken sleep.
Depression and Anxiety. Research has linked low magnesium to a higher risk of depression and anxiety. Magnesium affects key brain systems that regulate mood, including the NMDA and GABA receptors and hormones like cortisol and serotonin. Several clinical studies have found that magnesium supplementation can ease symptoms in people with low baseline levels.
Gastrointestinal Disorders
Early symptoms of magnesium deficiency often include reduced appetite, nausea, and occasional vomiting. These effects are nonspecific and frequently overlooked, particularly in individuals already experiencing decreased food intake due to weight loss diets or medications.
Ozempic-class drugs compounding the risk of magnesium deficiency through reduced intake, impaired absorption, and increased losses from vomiting or diarrhea.
Daily losses of magnesium
Magnesium losses happen through urine, feces, and sweat. On average, they amount to:
Urinary loss is the primary excretory route and ranges roughly from 70 to 120 mg per day in healthy adults, depending on dietary intake, kidney function, and hormonal regulation.
Fecal losses typically range from 20 to 40 mg per day, mostly representing unabsorbed dietary magnesium and endogenous secretions.
Sweat losses vary widely by individual and activity level but generally account for about 10 to 30 mg per day in sedentary individuals, potentially much higher during heavy physical activity or hot climates.
These losses establish the need to regularly replenish magnesium to maintain homeostasis, considering that adult dietary recommendations generally range between 310–420 mg/day.
More precise quantification depends on individual factors such as age, sex, diet, kidney function, and environmental conditions. Because magnesium participates in hundreds of biochemical reactions and is extensively regulated by renal conservation mechanisms, losses can fluctuate.
Prevention and Supplementation
The Recommended Dietary Allowance (RDA) for magnesium is 400–420 mg/day for adult men and 310–320 mg/day for adult women. This value is based on the replacement amount needed to accommodate daily losses, but doesn’t account for the rate of assimilation, quality of the supplement, extra excretion, and other factors.
Optimal Daily Allowance (ODA) is higher when under stress or during illness. Supplemental magnesium citrate or similar forms are recommended when clinical symptoms or dietary restrictions suggest insufficiency. Excess intake can cause diarrhea or, rarely, toxicity in patients with kidney dysfunction.
The Conezymated Once Daily Multi formula provides foundational magnesium, but additional supplementation may be necessary when symptoms arise or intake is low.
Vitamins Required for Assimilation of Magnesium
Magnesium absorption and utilization in the body depend on several factors, including the presence and status of specific vitamins that support its metabolism and physiological functions. The key vitamins involved are.
Vitamin D enhances magnesium absorption in the intestines. Adequate vitamin D status facilitates the active transport of magnesium across the intestinal mucosa. Deficiency of vitamin D may impair magnesium uptake, contributing to systemic mineral deficiencies.
Vitamin B6 (pyridoxine) influences magnesium metabolism at the cellular level. It acts as a coenzyme in many enzymatic reactions involving magnesium and supports magnesium transport into cells. The B6 deficiency can lead to increased magnesium excretion and reduced availability.
Folate (B9) and B12 contribute to overall metabolic health and enzymatic function, indirectly supporting mineral balance and magnesium utilization.
Vitamin K works synergistically with minerals, including magnesium, to regulate bone metabolism and vascular health. While its direct role in magnesium absorption is less defined, optimal vitamin K status supports magnesium-dependent processes in bone mineralization.
The Once Daily Multi formula includes coenzymated, bioactive forms of B vitamins, including B6, to enhance absorption and utilization, which may also improve magnesium metabolism indirectly. Ensuring adequate intake of these vitamins supports magnesium status and overall mineral homeostasis.
In summary, magnesium is a vital electrolyte and macromineral involved in enzymatic functions, neuromuscular stability, cardiovascular health, glucose metabolism, skeletal integrity, and psychological well-being.
Many of the conditions discussed above converge to make magnesium deficiency one of the most overlooked but widespread nutritional problems in both clinical and subclinical forms.
For people dependent on bottled or municipal water and anyone above 50, supplementation is the only reliable and most economical way to maintain adequate intake of magnesium.
Potassium Deficiency
Potassium (K) is an essential macromineral and electrolyte. It controls water balance inside all cells, supports nerve signals and muscle contractions, and maintains a steady heart rhythm. It also controls blood pressure regulation and pH balance.
Potassium (K⁺) and sodium (Na⁺) ions work are antagonists: sodium maintains water outside cells, potassium retains it inside. This ionic push-pull stabilizes cell volume. Without enough potassium, this balance breaks down.
When potassium is low, sodium is retained, increasing blood plasma volume and vascular resistance. Low potassium also increases vascular smooth muscle contraction and sympathetic activity, both of which elevate blood pressure even more.
Inside the body, potassium exists only in its ionic form (K⁺), dissolved in fluids. Over 98% of it is stored inside cells. Only a tiny fraction circulates in the blood, which makes blood tests a poor measure of total status. The kidneys excrete what the body doesn’t need, mostly through urine. Some is lost through sweat and stool. Like sodium, potassium must come in daily from outside sources.
Potassium deficiency is common in people who lose fluids with vomitting, diarrhea, use diuretics, or take medications that shift potassium out of the blood. It also happens in people who don’t eat enough potassium-containing food. Early symptoms include fatigue, weakness, cramps, dizziness, and irregular heartbeat.
Severe deficiency can cause paralysis, arrhythmias, or cardiac arrest. Hospitalized patients die from potassium deficiency every day — hypokalemia is reported to have an in-hospital mortality rate as high as 17%. The risks go up with high salt loss, dehydration, insulin use, magnesium deficiency, or digitalis.
Dietary Sources of Potassium
Potassium is present in almost all natural foods. The richest sources are animal-based: fish, red meat, liver, dairy, and eggs. These foods are dense in potassium and absorb well. It isn't surprising to understand why – the fluid inside every single cell is saturated with potassium.
Plant-based sources like potatoes, bananas, beans, and greens contain potassium too, but much of it is lost in cooking or poorly absorbed due to fiber and antinutrients. In the context of potassium, the most relevant antinutrients are:
Phytates (phytic acid). Found in legumes, whole grains, and seeds. They bind minerals and reduce bioavailability.
Oxalates. Present in spinach, beet greens, and some other vegetables. They form insoluble salts with minerals like calcium and magnesium, indirectly affecting potassium uptake.
Tannins. Found in tea, wines, whiskey, scotch, legumes, and some fruits. They can inhibit digestive enzymes and reduce the absorption of nutrients.
Low-potassium status is now widespread, thanks to modern food processing, water treatment, and chronic drug use. Most people who avoid salt also avoid the foods that contain and retain potassium. And those who lose salt through sweat, urine, or illness usually lose potassium with it as well.
Fresh cucumber juice made with skins and salt to taste is one of the highest, cleanest, and easiest-to-assimilate sources of potassium. It contains no sugar, no fiber, and no antinutrients. Organic is best, especially if juicing with skins.
Hypokalemia (low blood potassium). Defined as serum potassium levels below 3.5 mmol/L. Most cases result from losses through diuretics, vomiting, diarrhea, or inadequate intake.
Fatigue and muscle weakness. Reduced intracellular potassium impairs nerve conduction and muscle fiber responsiveness, leading to sluggishness, weakness, and low exercise tolerance.
Muscle cramps. Potassium imbalance disrupts neuromuscular control, resulting in involuntary contractions, cramps, and twitching, particularly in the legs.
Constipation and intestinal sluggishness. Smooth muscle activity in the gut depends on potassium. Deficiency slows peristalsis and increases the risk of constipation.
Dizziness and lightheadedness. Low potassium can reduce blood flow to the brain due to reduced cardiac output or vascular instability, causing dizziness, especially when standing up.
Heart palpitations and arrhythmias. Potassium is critical for electrical activity in cardiac muscle. Deficiency destabilizes the heartbeat, leading to irregular rhythms or a racing heart.
Severe complications. In advanced cases, hypokalemia may lead to flaccid paralysis, life-threatening arrhythmias, or respiratory arrest due to impaired muscle contraction.
Insulin resistance and poor glucose tolerance. Potassium is required for insulin secretion from pancreatic beta cells. Deficiency impairs glucose uptake and contributes to metabolic dysfunction.
Elevated blood pressure and vascular tension. Low potassium reduces the ability of arteries to relax, increasing vascular resistance and raising blood pressure, especially when sodium intake is high.
Cardiac instability in sensitive patients. Individuals with heart disease or those taking digoxin, loop diuretics, or corticosteroids face a higher risk of arrhythmias and sudden cardiac events when potassium is low.
Potassium Daily Requirements
The Recommended Dietary Allowance (RDA) for potassium in the United States is 3,400 mg/day for adult men and 2,600 mg/day for adult women. These values reflect minimal intake levels required to prevent overt deficiency in healthy individuals.
An Optimal Daily Allowance (ODA) for potassium is not officially established, but clinical and observational data suggest that daily intake between 4,000–6,000 mg may better support cardiovascular, renal, and neuromuscular health in the general population, especially under conditions of stress, physical activity, or elevated sodium intake.
Potassium needs vary depending on body size and lean muscle mass, salt intake (higher intake requires more potassium), physical activity and sweat loss, use of diuretics or laxatives, chronic illnesses, and digestive disorders.
Potassium supplements in doses above 99 mg require a prescription because they can cause gastrointestinal irritation and cardiac complications. This regulation is based on the following concerns:
Risk of gastrointestinal injury. Higher doses of oral potassium salts like potassium chloride have been associated with irritation, ulcers, or perforation in the esophagus, stomach, or small intestine.
Cardiac risks from overdose. Potassium affects the heart's electrical conduction. Inappropriate use in individuals with kidney impairment, heart disease, or those taking potassium-sparing drugs can cause hyperkalemia and lead to fatal arrhythmias.
Lack of prescriber oversight. The 99 mg cap ensures that higher-dose potassium supplements such as K-Dur or Micro-K, which provide 600–750 mg per tablet or capsule, are only used by prescription.
Similar risks do not apply to food sources because potassium in whole foods exists in natural ionic form, accompanied by water and other nutrients that slow absorption and support renal regulation.
Recommendations
Potassium is critical to heart, muscle, nerve, and kidney function. Most people with low potassium don’t know it until they crash. You cannot count on blood tests alone, and you cannot fix a deficiency with a banana. The best sources are animal-based and unprocessed. Vegetables help, but only when cooked and combined with salt and fat.
Dietary fat improves the absorption of fat-soluble vitamins A, D, E, and K, which, in turn, enhances the assimilation of minerals, including potassium and magnesium. Without fat, many nutrients in vegetables pass through the digestive tract unabsorbed.
Potassium supplements work but should be used cautiously, especially in people with poor kidney function. For everyone else, the goal is simple: eat real food, get enough salt, and don’t deplete your body with too much water, drugs, and processed foods.
Sodium Deficiency
Sodium (Na) is an essential macromineral and electrolyte. It's present in ionic form (Na+) in all extracellular fluids and regulates their volume, acid-base balance, nerve transmission, and muscle contraction. It also helps maintain blood plasma osmolality and is tightly regulated by the kidneys through hormonal control mechanisms involving aldosterone and antidiuretic hormone.
Sodium in the body exists exclusively as a positively charged ion (Na⁺) dissolved in fluids, not as elemental sodium or dry salt crystals. It circulates primarily in blood plasma and interstitial fluid, where it helps maintain osmotic pressure, electrical gradients, and the movement of water across cell membranes. Its ionic form is essential for nerve conduction, muscle contraction, and the regulation of extracellular fluid volume.
The term “sodium” is commonly used interchangeably with “salt” in public health messaging and food labeling. This usage is grossly incorrect. Salt refers to sodium chloride (NaCl), which is about 40% sodium and 60% chloride by weight.
Using sodium as a synonym for salt intentionally misrepresents the role of chloride in fluid regulation, overstates the sodium content in foods, and creates confusion about actual dietary requirements. It also promotes the false idea that salt is inherently harmful, instead of acknowledging its essential role in hydration, stomach acid production, and cellular health.
Sodium is lost through urine, sweat, and feces. The kidneys regulate urinary excretion of sodium in response to hormonal signals and changes in blood volume or osmolality.
During heavy sweating, high fever, or prolonged physical exertion, a significant amount of sodium can be lost through the skin with perspiration. Gastrointestinal losses from diarrhea and vomiting can also deplete sodium rapidly. In all cases, sodium loss leads to a corresponding loss of water, increasing the risk of dehydration, muscle cramps, and neurological symptoms.
Unlike minerals like calcium or iron, sodium is not stored in a dedicated reserve within the body. It circulates in extracellular fluid and must be continuously replenished through diet to maintain physiological balance.
Because the body doesn't store sodium, even brief deficits from low intake or loss can compromise fluid balance, nerve function, and blood pressure regulation. For this reason, daily dependence on diet is constant.
Overhydration and excessive consumption of foods or substances with diuretic properties can significantly disrupt sodium balance by accelerating its loss through urine. When large volumes of low-sodium fluids are consumed, especially plain water, the kidneys may excrete sodium faster than it can be replaced, diluting blood sodium levels and increasing the risk of hyponatremia.
This effect is compounded by foods and beverages with natural diuretic effects, such as caffeine-containing drinks, alcohol, watermelon, cucumber, celery, and asparagus. In individuals with already low sodium intake or increased fluid losses, these factors can quickly lead to symptoms of sodium depletion, including weakness, confusion, dizziness, and muscle cramps.
Hyponatremia can be life-threatening, particularly when sodium levels drop rapidly or fall below critical thresholds. Severe cases may lead to cerebral edema, seizures, respiratory arrest, coma, and death.
This is one reason intravenous fluid infusion—typically isotonic saline—is the first intervention administered in most medical emergencies. It stabilizes blood volume, restores circulating sodium, and prevents further deterioration from fluid-electrolyte imbalances, especially in cases involving trauma, dehydration, or systemic shock.
Sodium by itself does not cause elevated blood pressure. In healthy individuals, excess sodium is efficiently excreted through the gastrointestinal tract—primarily via the stomach and colon—as well as through the kidneys.
The body maintains tight hormonal control over sodium balance, and elevated blood pressure typically results from impaired renal sodium handling, hormonal dysregulation, or coexisting factors such as low potassium, low magnesium, dehydration, or vascular dysfunction. Blanket sodium restriction ignores these complexities and often leads to unintended health consequences.
Dietary Sources of Sodium
Sodium is naturally present in small amounts in most whole foods, including meat, seafood, dairy, and vegetables. The majority of dietary sodium in modern diets comes from added salt (sodium chloride), whether used in cooking or added during food processing. Processed foods, such as breads, sauces, deli meats, canned goods, and packaged snacks, contribute disproportionately.
Individuals following low-sodium or unprocessed diets may inadvertently fall below physiologic sodium needs, especially in hot climates, during physical exertion, or while using medications that increase sodium loss.
Hyponatremia, or low blood sodium, is a primary form of deficiency. This condition causes headache, nausea, confusion, muscle cramps, weakness, and fatigue. In severe cases, it may cause seizures, coma, and respiratory arrest.
Sodium losses result from sweating, diarrhea, vomiting, overhydration, or restrictive low-sodium diets. Diuretics, laxatives, SSRIs, antipsychotics, and oxcarbazepine cause drug-induced sodium loss.
Sodium Toxicity
I refer to "salt" here because it is the only path of sodium into the body in large amounts. The estimated lethal dose of salt (sodium chloride) in humans is approximately 0.2 to 0.5 grams per kilogram of body weight. This ratio translates to 14 to 35 grams of salt (about 2.5 to 6 teaspoons) for a 70 kg (154 lb) adult, consumed in a short time frame.
Individual tolerance to salt varies depending on hydration status, renal function, and rate of ingestion. Death from salt poisoning (acute hypernatremia) generally results from rapid fluid shifts in the brain, leading to cerebral edema, seizures, and respiratory failure.
Documented cases of fatal salt ingestion often involve children, due to lower body weight, forced salt consumption, as in child abuse cases, and salt challenges or internet “pranks”, where individuals consume tablespoons of salt at once. In hospital settings, serum sodium levels above 160–170 mmol/L are considered critically dangerous.
Sodium Daily Requirements
There is no RDA for sodium because it is considered a nutrient with a low requirement and a high risk of excess in modern diets. These values reflect the minimum needed to maintain physiological function under typical conditions—not optimal levels for everyone.
The daily Adequate Intake (AI) for sodium is set at:
Ages 19–50. Adequate Intake (AI) is 1,500 mg of sodium per day (≈ 3.8 grams of salt).
Ages 51–70. AI is 1,300 mg of sodium per day (≈ 3.3 grams of salt).
Over 70. AI is 1,200 mg of sodium per day (≈ 3.0 grams of salt).
The Tolerable Upper Intake Level (TUL) for sodium is 2,300 mg per day for all adults, equivalent to roughly 5.8 grams of salt.
Let's review the same for children:
Infants 0–6 months: 110 mg sodium/day (≈ 0.3 grams salt).
Infants 7–12 months: 370 mg sodium/day (≈ 0.9 grams salt).
Children 1–3 years: 800 mg sodium/day (≈ 2.0 grams salt).
Children 4–8 years: 1,000 mg sodium/day (≈ 2.5 grams salt).
Children 9–13 years: 1,200 mg sodium/day (≈ 3.0 grams salt).
Adolescents 14–18 years: 1,500 mg sodium/day (≈ 3.8 grams salt).
Infants get their salt from breast milk, which underscores the importance of adequate salt intake for nursing mothers. This also explains why many breastfeeding women experience strong salt cravings. Infant formulas are properly adjusted for sodium content by manufacturers.
These benchmarks reflect the minimum necessary to maintain essential physiological functions under average conditions. They are not individualized or optimized for people with higher losses due to sweat, illness, or certain diets.
Recommendations
Sodium deficiency is rare in the general population consuming processed foods, but can occur in individuals following very low-salt diets, those using diuretics, or those with high fluid losses. In such cases, symptoms may be mistakenly attributed to dehydration or fatigue rather than sodium imbalance.
Routine sodium supplementation is unnecessary without a clear medical indication, but individuals with excessive fluid intake or low-salt diets should remain alert to early signs of sodium depletion.
To learn more about this super controversial and deliberately misrepresented subject, read my guide 44 Serious Disorders Caused by Salt Deficiency. Yes, forty-four. Most of what you've heard about sodium and salt is likely a lie or fraud. This guide may extend your life the same way it extended mine.
Chloride Deficiency
Just like sodium, chloride (Cl) is an essential macromineral and the main extracellular anion in the body. It remains in close balance with sodium, working together to regulate fluid volume, osmotic pressure, and acid-base balance.
Although chloride has several important physiological functions, it's rarely discussed independently of sodium. As a result, many people don't realize how essential chloride is on its own.
In the body, chloride is found only as a negatively charged ion (Cl⁻) in the fluid outside of cells. It moves through blood plasma and between cells, balancing the positive charges from ions like sodium and potassium.
Chloride is absorbed in the small intestine and is mostly excreted by the kidneys, with smaller amounts leaving the body through sweat and stool. Like sodium, chloride isn't stored in the body and needs daily replenishment with food.
Chloride is almost exclusively consumed as part of sodium chloride (NaCl)—table salt, which is 60% chloride by weight. Because salt is the main dietary source of both sodium and chloride, reductions in salt intake inevitably reduce chloride intake as well.
Chloride loss occurs primarily through urine, which is tightly regulated by the kidneys. Additional losses occur from sweating, blood loss, vomiting, and nasogastric suction (removal of stomach fluids via the tube inserted through the nose) in hospitalized patients. Because chloride is a key component of hydrochloric acid, persistent vomiting or gastric drainage can cause substantial chloride depletion.
Loss of chloride leads to a rise in blood bicarbonate levels and results in metabolic alkalosis, a dangerous shift in pH that impairs oxygen delivery, enzyme function, and overall metabolic stability.
Like sodium, chloride is not stored in reserve and is entirely dependent on dietary intake. If you consume little or no salt, especially during long heat exposure such as sauna or on the beach, or periods of fluid loss related to diarrhea or vomitting, you are at increased risk of chloride deficiency. Diuretics, laxatives, and corticosteroids may further deplete chloride, particularly when combined with low dietary intake or high water consumption.
Hypochloremia (low blood chloride) is the clinical name for chloride deficiency. It's often seen in hospitalized patients with prolonged vomiting, diuretic use, and adrenal insufficiency. Symptoms may include fatigue, muscle weakness, shallow breathing, confusion, and slowed digestion due to reduced stomach acid. These symptoms are often misattributed to other causes unless chloride is specifically measured and addressed.
Ions of chloride are essential for sustaining proper stomach acidity. Without sufficient chloride, the body cannot maintain adequate hydrochloric acid (HCl) levels in the stomach. Low stomach acid impairs the digestion of protein, sterilization of viruses, bacteria, and parasites in food, and the absorption of minerals.
Dietary Sources of Chloride
Chloride is most abundant in table salt (sodium chloride), which supplies both sodium and chloride in a fixed ratio. Other common sources include sea salt, salted meats, canned goods, pickled foods, cheese, eggs, and seafood. Naturally occurring chloride is also present in celery, tomatoes, olives, lettuce, and seaweed. Individuals on low-salt diets or using only unfortified salt substitutes (e.g., potassium chloride) may not get enough chloride to meet physiological demands. Unlike sodium, which receives public attention and regulatory monitoring, chloride intake is rarely tracked or discussed—even in clinical practice.
Primary Deficiencies of Chloride
Hypochloremia (low serum chloride). Characterized by symptoms such as fatigue, muscle weakness, shallow or depressed breathing, confusion, and slowed digestion. It often develops due to vomiting, nasogastric suction, chronic diarrhea, use of diuretics, adrenal insufficiency, or excessive fluid intake that dilutes serum electrolytes.
Low stomach acid (hypochlorhydria). Inadequate chloride can impair the stomach’s ability to produce hydrochloric acid (HCl), which is essential for protein digestion and mineral ionization. This condition increases the risk of nutrient deficiencies and gastrointestinal infections due to reduced acidity.
Metabolic alkalosis. Chloride depletion from vomiting or use of certain diuretics can result in a compensatory increase in blood bicarbonate levels, leading to metabolic alkalosis—a serious disturbance in acid-base balance that impairs oxygen delivery and enzyme function.
Electrolyte imbalances. A lack of chloride, especially when combined with low sodium intake, can disrupt overall electrolyte stability. This is common in individuals following salt-restricted diets, consuming excess water, or receiving salt-free IV fluids, all of which may deplete chloride reserves without clinical recognition.
Recommendations
Chloride is a vital yet underappreciated mineral required for digestion, hydration, acid-base stability, and fluid regulation. Deficiency is rare under normal dietary conditions but may occur with salt-restricted diets, prolonged vomiting, or excessive diuretic use.
Because most chloride comes from dietary salt, intentional salt restriction—especially when combined with other risk factors—can lead to hypochloremia and associated complications. As with sodium, routine supplementation is not necessary for most people, but chloride intake should not be overlooked in discussions about electrolyte balance, hydration, or digestion. Salt used in moderation remains the safest and most practical source of both sodium and chloride.
Phosphorus Deficiency
Phosphorus (P) is an essential macromineral found in every cell of the body. It is the second most abundant mineral after calcium and is critical for the formation of bones and teeth, where about 85% of total body phosphorus is stored as hydroxyapatite crystals.
The remaining phosphorus circulates in soft tissues and plays a central role in energy production (as part of ATP), DNA and RNA structure, cellular signaling, and acid-base buffering. Despite its importance, phosphorus deficiency from inadequate dietary intake is rare in individuals consuming a modern, protein-rich diet.
Phosphorus exists in the body almost entirely as phosphate (PO₄³⁻), its active ionic form. It is absorbed in the small intestine and regulated by the kidneys, parathyroid hormone (PTH), and vitamin D.
Unlike sodium or chloride, phosphorus is found in high concentrations in a wide range of both animal and plant foods. Because of this, most individuals easily meet their needs without supplementation. In fact, excessive intake—particularly from food additives and cola beverages—is far more common than deficiency.
True phosphorus deficiency (hypophosphatemia) is usually secondary to underlying medical conditions rather than poor dietary intake. Among its primary causes are alcoholism, diabetic ketoacidosis, refeeding syndrome (restarting nutrition after the fast), hyperparathyroidism, or chronic use of antacids containing aluminum or magnesium, which bind phosphate in the small intestine. In all of these cases, serum phosphate levels fall, affecting energy metabolism, oxygen delivery, bone integrity, and muscle and nerve function.
Moderate to severe hypophosphatemia causes bone pain, muscle weakness, fatigue, irritability, and impaired immune function. In critical cases, it may also cause arrhythmias, hemolysis, neurological impairment, and the failure of respiratory muscles.
Dietary Sources of Phosphorus
Phosphorus is plentiful in meat, poultry, fish, dairy, eggs, legumes, nuts, seeds, and whole grains. It is also present in many processed foods and beverages as phosphate-based additives. These additives are highly bioavailable and often push phosphorus intake far beyond recommended levels.
Phosphorus from animal sources is generally better absorbed than from plant sources, where it is bound to phytates, the principal storage form of phosphorus in many plant tissues.
The Recommended Dietary Allowance (RDA) for phosphorus, as set by the Institute of Medicine, is:
Adults (19 years and older): 700 mg per day.
Pregnant and lactating women (19+): 700 mg per day.
Children and adolescents (9–18 years): 1,250 mg per day.
Children (1–8 years): 500 mg per day.
Infants (7–12 months, Adequate Intake): 275 mg per day.
Infants (0–6 months, Adequate Intake): 100 mg per day.
The average Western diet easily exceeds those requirements without supplementation.
The much higher phosphorus RDA for children and adolescents between 9 and 18 years reflects the increased demand during the most intensive stage of bone mass development.
Recommendations
Phosphorus deficiency is rare in healthy individuals consuming a balanced diet. It becomes clinically significant mostly in the context of disease, malnutrition, or prolonged medical treatment. Because phosphorus is so widely available in food, especially animal protein and processed items, routine supplementation is unnecessary.
Excess intake of phosphorus from additives and supplements is a more common concern among individuals with kidney disease because its retention can contribute to vascular calcification and bone disease.
Sulfur Deficiency
Sulfur (S) is an essential macromineral that plays a structural and metabolic role in the body, though it is rarely discussed in isolation. It is present in the body as part of methionine and cysteine — two sulfur-containing amino acids which are vital for protein synthesis, enzyme activity, antioxidant defense, and detoxification. It's also a key component of thiamine, biotin, pantothenic acid, glutathione, and taurine.
These biologically active forms are absorbed, metabolized, and integrated into structural proteins, enzymes, and metabolic pathways. The body relies entirely on organic sulfur compounds from dietary sources to meet its physiological needs.
Sulfur contributes to the integrity of connective tissue, skin, hair, nails, and cartilage via disulfide bonds in keratin and collagen.
Sulfur deficiency from dietary sources is rare in humans and typically occurs only in the context of severe protein malnutrition. Since methionine is an essential amino acid, diets devoid of adequate animal protein may reduce sulfur availability.
Vegan or vegetarian diets can meet sulfur needs if they include adequate legumes, nuts, and seeds, but diets limited in total protein can fall short over time.
Sulfur is lost through urine and bile, and to a lesser extent through sweat and shedding of skin and hair. There is no known physiological mechanism for sulfur storage, so its status depends entirely on consistent intake of sulfur-rich amino acids and vitamins.
A marginal deficiency may contribute to impaired detoxification, poor wound healing, brittle hair and nails, and joint or connective tissue complaints, but there is no widely recognized clinical syndrome of isolated sulfur deficiency in humans.
Dietary Sources
Sulfur is derived almost entirely from dietary protein, particularly from methionine and cysteine. Rich sources include meat, poultry, fish, eggs, dairy, legumes, nuts, and seeds.
Cruciferous vegetables (e.g., broccoli, cabbage, Brussels sprouts, garlic, onions) also contain sulfur-containing compounds such as sulforaphane and allicin, which contribute to detoxification processes in the liver.
While these compounds are biologically active, they are not a substitute for sulfur-containing amino acids and do not meaningfully correct sulfur deficiency on their own.
Primary Sulfur Deficiencies
There is no formally established disease entity defined as primary sulfur deficiency. However, inadequate sulfur intake can impair key metabolic functions from the following factors:
Severe protein malnutrition. Individuals with chronically low protein intake related to eating disorders, chronic illness, or extreme dietary restrictions may not consume enough sulfur-containing amino acids to meet metabolic demands.
Low intake of methionine and cysteine. Methionine and cysteine are the main dietary sources of sulfur. Diets that exclude animal proteins or do not include plant-based alternatives rich in these amino acids may result in insufficient sulfur availability for the synthesis of structural and functional proteins.
Restrictive diets. Diets centered on refined carbohydrates, ultra-processed foods, or restrictive meal plans may lack both the quantity and diversity of amino acids necessary to support sulfur metabolism.
Impaired detoxification and cellular protection. Sulfur is required for the synthesis of glutathione, a critical compound involved in neutralizing reactive byproducts of metabolism and environmental exposures. Sulfur deficiency may impair the body’s ability to maintain cellular integrity and detoxification pathways.
Recommendations
Sulfur is essential for structural proteins, metabolic function, and cellular defense, but true deficiency is exceedingly rare outside of protein malnutrition or restrictive diets.
Supplementation isn't required when consuming adequate protein from animal or plant sources. For practical purposes, a balanced diet ensures adequate sulfur status without the need for monitoring or intervention.
Frequently Asked Questions 
Q. How does my water filtration system affect my mineral intake?+
Water filtration systems, especially reverse osmosis (RO), distillation, and certain high-efficiency carbon filters, remove not only contaminants but also naturally occurring minerals such as calcium, magnesium, and trace elements.
Regular consumption (drinking or cooking) of demineralized water may reduce overall mineral intake, particularly if your diet is already low in these nutrients. Over time, this can contribute to subclinical deficiencies, especially of magnesium and calcium.
To offset these losses, it’s important to use targeted supplementation. Some systems allow for post-filtration remineralization, but most do not. Even if yours does, it’s much more reliable and probably less expensive to add supplements to your diet than to ‘supplement’ your water.
Q. Can I get all of the minerals and trace elements from the diet and drinking water in Chicago?+
In theory, a well-balanced diet could supply most essential minerals and trace elements. However, in practice, this depends on food quality, dietary habits, and local water composition.
Chicago’s municipal water is treated and contains added fluoride but relatively low levels of naturally occurring minerals like magnesium and calcium. It cannot be relied on as a significant mineral source. Modern diets, even when varied, often fall short in key trace elements such as magnesium, zinc, iodine, selenium, and boron due to food processing, agricultural depletion, and selective eating patterns.
While it’s possible to meet mineral needs through diet alone, doing so consistently is uncommon. Supplementation helps ensure adequate and stable intake, especially for nutrients that are marginal or missing in local water and food sources.
This answer applies to any other major metropolitan area in the United States. If you want a more specific assessment, you can also find your local water analysis report by checking the website of your city’s water utility or visiting the EPA’s Consumer Confidence Report (CCR) database at www.epa.gov/ccr.
Q. Is water in New York as good as I've been reading?+
New York City’s tap water is widely regarded as some of the best municipal water in the United States. It originates from protected reservoirs in the Catskill and Delaware watersheds and is known for its low levels of pollutants, favorable taste, and relatively soft mineral content.
However, while the source water is high quality, it is still treated with chlorine and may pick up trace contaminants from aging pipes or local infrastructure. It contains only modest levels of essential minerals like calcium and magnesium and should not be relied on as a meaningful source of daily mineral intake.
So while New York tap water is safe and well-managed, supplementation is still necessary to meet full mineral requirements.
Q. Is it realistic to get all of the minerals and trace elements from supermarket food?+
No. While supermarket food can provide calories, protein, and some essential nutrients, it often falls short in supplying adequate amounts of many minerals and trace elements. Modern agricultural practices, soil depletion, food processing, and long storage times reduce the mineral content of both plant and animal products. Packaged and prepared foods are especially low in magnesium, potassium, zinc, iodine, selenium, and boron.
Even with careful planning, it is difficult to meet full mineral requirements consistently from supermarket food alone. Supplementation helps close the gap and maintain stable, physiologically sufficient intake.
Supplementation costs a fraction of what it would take to obtain equivalent mineral levels from food alone, and it helps avoid carbohydrate overload, overeating, cooking time, and potential contamination from industrial food sources.
Q. We get our water from a private well. How does water softening affect mineral and trace element content?+
Water softening systems that use ion exchange remove calcium and magnesium by replacing them with sodium or potassium ions. This process significantly reduces the water’s hardness but also eliminates two important dietary minerals.
Trace elements, such as zinc, copper, or iron, aren’t targeted by the softening process, and may still be present, depending on the composition of the source water.
If softened water is your primary drinking source, you should account for the loss of calcium and magnesium, especially if dietary intake is borderline. Supplementation may be needed to maintain adequate levels.
My best advice — consider testing your well water before and after softening at a certified laboratory to assess mineral levels and ensure safe overall composition.
Q. Can physical activity or athletic training increase my mineral requirements?+
Yes. Physical activity—especially when frequent or intense—increases the body’s demand for several minerals.
Sweating leads to losses of sodium, chloride, potassium, magnesium, and zinc. Exercise also accelerates tissue turnover and repair, increasing requirements for calcium and magnesium to support muscle function and bone remodeling. Minerals like selenium, copper, and manganese are needed in higher amounts to support energy metabolism and enzymatic activity under physical stress.
Without adequate replacement, these deficits can lead to fatigue, muscle cramps, reduced performance, and higher risk of injury.
Q. Does drinking a lot of coffee, tea, or alcohol change my need for certain minerals?+
Yes. Regular or high intake of coffee, tea, and alcohol can increase your requirements for several essential minerals due to their effects on absorption, excretion, and metabolism.
Coffee and tea act as mild diuretics and increase urinary excretion of magnesium, calcium, sodium, and potassium. They also contain tannins and phytates, which can inhibit the intestinal absorption of non-heme iron and zinc—especially when consumed in large amounts or alongside meals. Over time, these effects may reduce overall mineral availability, particularly in individuals with marginal dietary intake.
Alcohol has a stronger diuretic effect and further increases urinary losses of magnesium, potassium, and zinc. It also impairs active transport and absorption of calcium and other nutrients in the small intestine. Chronic alcohol consumption can lead to sustained mineral depletion, contributing to muscle weakness, fatigue, poor wound healing, and reduced bone density. In severe cases, long-term alcohol use can result in clinically significant deficiencies and structural damage.
While moderate consumption may not pose problems for healthy individuals with a balanced diet and mineral-rich water, high or frequent intake raises the risk of insufficiencies. Supplementation may be necessary to offset these cumulative losses and support metabolic balance.
Q. How do popular diets like keto, vegan, and intermittent fasting affect my mineral status?+
All restrictive or mono-diet, including ketogenic, vegan, and intermittent fasting, require supplementation. Without it, you risk hidden or progressive deficiencies for the following reasons:
Ketogenic diets restrict or eliminate many fruits, vegetables, and legumes, reducing dietary intake of potassium, magnesium, and calcium. The diuretic effect of ketosis further increases urinary losses of sodium, potassium, and magnesium, raising the risk of electrolyte imbalance, muscle cramps, and fatigue.
Vegan and plant-based diets limit or exclude animal-derived sources of highly bioavailable minerals. These diets typically fall short in iron, zinc, calcium, iodine, and selenium due to lower concentrations in plants and the presence of absorption inhibitors like phytates and oxalates. Even with diverse food choices, long-term adherence without supplementation can lead to subclinical or overt deficiencies.
Intermittent fasting reduces total food volume, which lowers overall mineral intake. If the eating window is narrow and the diet is not mineral-dense, it becomes difficult to meet daily requirements for magnesium, potassium, calcium, and trace elements.
In all cases, mineral supplementation is critical to maintain physiological balance and prevent deficiency-related symptoms or long-term complications.
Q. Will periods of fasting or juice cleanses impact my mineral balance?+
Yes. Fasting and juice cleanses reduce or eliminate intake of foods that provide essential minerals. This practice quickly affects electrolyte balance and metabolic stability.
Prolonged fasting, typically beyond 24 to 48 hours, can accelerate the depletion of sodium, chloride, potassium, magnesium, and phosphate. As these minerals are continuously lost through urine and sweat, their absence from the diet increases the risk of fatigue, muscle cramps, dizziness, and other signs of electrolyte imbalance.
Juice cleanses provide minimal amounts of minerals, especially sodium and protein-bound trace elements, and may also contain substances like oxalates or fructose that interfere with mineral retention.
Q. Are “natural” or “food-based” mineral supplements better absorbed than synthetic ones?+
No. All mineral supplements, whether labeled “natural,” “food-based,” or “synthetic,” are produced using chemical and thermal processing.
The only truly natural sources of minerals are soil, water, and plants. To make any of them usable in supplements, manufacturers must extract, purify, and stabilize the minerals using industrial methods.
Unprocessed or minimally processed “natural” supplements often have inconsistent dosing and may carry environmental contaminants or trace toxins from their source materials.
In contrast, high-quality synthetic supplements contain purified mineral salts or chelates, such as citrates, ascorbates, glycinates, or picolinates, with well-established bioavailability and consistent performance. These forms are widely studied, well tolerated, and reliably absorbed.
Our supplements are specifically formulated with these optimized forms to ensure purity, stability, and efficient metabolic use.
Q. How do antacids, antibiotics, or common prescription medications impact mineral absorption?+
Certain medications can significantly interfere with mineral absorption, metabolism, or increase mineral losses:
Antacids and proton pump inhibitors (PPIs) reduce stomach acid, which is necessary for dissolving and absorbing minerals like calcium, magnesium, and iron, leading to decreased bioavailability.
Antibiotics can disrupt gut microbiota, impairing synthesis of vitamin K and B vitamins and affecting mineral absorption indirectly. Some antibiotics can also bind minerals in the gut, reducing their uptake.
Diuretics increase urinary excretion of minerals such as potassium, magnesium, and calcium, potentially causing deficiencies.
Cholesterol-lowering drugs (statins) may affect coenzyme Q10 and indirectly influence mineral-dependent metabolic pathways.
Because many chronic conditions require long-term medication use, it’s important to monitor mineral status and consider supplementation when appropriate.
Corticosteroids reduce calcium absorption in the intestines and increase calcium losses through urine. They also promote sodium retention and potassium excretion. These effects contribute to bone demineralization and raise the risk of osteoporosis with long-term use.
Hormonal therapies, including thyroid hormones and estrogen, also affect mineral balance. Excess thyroid hormone increases the turnover of calcium and phosphorus, potentially leading to bone loss. Estrogen influences both calcium metabolism and magnesium levels.
Stimulant laxatives, when used regularly, accelerate gastrointestinal transit time and reduce absorption of minerals such as calcium, magnesium, and zinc. Chronic use can also cause significant losses of potassium and other electrolytes.
Chelating agents like penicillamine and EDTA bind divalent and trivalent metal ions—including calcium, magnesium, zinc, iron, and copper—making them unavailable for absorption. While these drugs are used therapeutically, they can cause mineral depletion if not properly managed.
Certain anticonvulsants, including phenytoin and phenobarbital, increase the breakdown of vitamin D in the liver. This outcome reduces calcium absorption and can lead to hypocalcemia and secondary hyperparathyroidism over time.
Oral contraceptives have been shown to reduce serum magnesium levels and may also alter zinc and copper status with prolonged use.
Q. How does gut health or history of digestive disorders change my mineral requirements?+
Digestive disorders such as celiac disease, Crohn’s disease, inflammatory bowel disease, or chronic diarrhea can impair the absorption of many minerals, including calcium, magnesium, iron, zinc, and selenium. Damage to intestinal lining reduces the surface area available for mineral uptake, leading to deficiencies despite adequate intake.
Dysbiosis (missing gut bacteria) can also interfere with micronutrient metabolism. Additionally, prior surgeries like gastric bypass can reduce stomach acid and digestive enzymes, further limiting mineral assimilation. People with these conditions often have increased mineral requirements.
Q. Do genetic differences (such as MTHFR mutations) influence mineral metabolism or needs?+
Genetic variations can affect how minerals are utilized in the body. For example, MTHFR mutations primarily impact folate and B-vitamin metabolism, but since many enzymatic processes depend on minerals like magnesium as cofactors, mineral status can indirectly influence genetic expression and metabolic pathways.
Q. How do I get tested for MTHFR mutations?+
To test for MTHFR mutations, doctors usually order a blood or saliva-based DNA test. Common lab methods include PCR-based genotyping or next-generation sequencing panels.
If part of a larger panel, additional codes may apply, depending on the lab's protocol and the clinical context (e.g., thrombophilia, cardiovascular risk, or neurological disorders). Always verify with the performing lab or insurance provider for up-to-date billing practices and medical necessity documentation.
Q. Can I get too much of certain trace minerals? What are the risks of long-term low-level excess?+
Yes. Even trace minerals can become toxic when consumed in excess, particularly over long periods.
Chronic copper overload may lead to liver damage and neurological symptoms. Excess selenium can cause gastrointestinal distress, hair loss, fatigue, and peripheral nerve dysfunction. Iron accumulation—whether from supplementation or metabolic disorders—can cause tissue injury, especially in the liver, heart, and pancreas.
Low-level excess from daily supplements or environmental exposure may result in subtle but cumulative effects, including metabolic disruption and organ stress. These imbalances often go undetected until symptoms emerge.
To reduce risk, it is important to stay within established upper intake levels. Long-term use of high-dose supplements should be monitored with periodic blood testing.
The safest and most efficient approach is to use a well-formulated, balanced multivitamin such as our Conezymated Once Daily Multi formula, rather than taking individual minerals separately in high doses. This approach helps prevent both deficiency and inadvertent excess.
Q. Is there a way to detect hidden or early-stage mineral deficiencies before symptoms appear?+
Yes. Several laboratory tests can identify mineral imbalances or insufficiencies before clinical symptoms develop.
Early detection allows for timely dietary adjustments or supplementation. For best results, test outcomes should be interpreted alongside clinical findings and other nutritional markers.
Serum or plasma measurements can assess levels of key minerals such as calcium, magnesium, zinc, copper, and selenium. Red blood cell mineral testing offers a more stable reflection of long-term status for certain nutrients, particularly magnesium and zinc.
A 24-hour urine analysis can evaluate mineral excretion and help assess overall balance and retention. Urine tests assess recent losses but can fluctuate widely depending on intake, hydration, and kidney function.
Hair mineral analyses are sometimes used but have limitations. Hair mineral testing reflects mineral content over weeks to months and can be affected by external contamination, hair treatments, and individual variability, reducing reliability.
Q. Do mineral status or requirements change with aging, menopause, or chronic illness?+
Yes. Mineral needs and status often change with age, hormonal shifts, and chronic disease.
Aging reduces digestive efficiency and lowers the absorption of minerals such as calcium, magnesium, and zinc. Menopause accelerates bone loss, increasing the demand for calcium and magnesium in particular.
Chronic conditions—including kidney disease, gastrointestinal disorders, and diabetes—can impair absorption, increase urinary or fecal losses, or alter mineral metabolism. Medication use, which is common in older adults, may further disrupt mineral balance.
After age 50, supplementation becomes the only consistent and reliable method of preventing mineral insufficiencies.
Q. Are specialized mineral forms like chelates, colloids, or liposomals worth the extra cost?+
Some specialized forms of minerals can offer advantages in absorption, tolerability, or effectiveness, depending on individual needs.
Chelated minerals—where the mineral is bound to an amino acid, such as magnesium glycinate or zinc picolinate—are often better absorbed and cause fewer gastrointestinal side effects than inorganic forms like oxides or carbonates.
Liposomal mineral formulations use phospholipid vesicles to enhance cellular delivery. While they may improve bioavailability, they are typically more expensive and are not necessary for most individuals with normal digestive function.
Colloidal minerals, often marketed as plant-derived or water-suspended particles, have inconsistent composition and lack strong evidence for superior absorption. Their safety and efficacy vary by source.
Whether the added cost is justified depends on your digestive capacity, symptom profile, and clinical needs. For individuals with absorption issues or sensitivity to standard forms, specialized formulations may provide measurable benefit.
Q. Can minerals from topical sources—such as creams, baths, or sprays—meaningfully contribute to my intake?+
Topical mineral products, including magnesium sprays, oils, and bathing salts, may provide localized effects such as muscle relaxation or skin conditioning. However, their contribution to systemic mineral status is limited.
Skin absorption of minerals is generally low and not well established in clinical research. While some absorption may occur—particularly during prolonged exposure, such as in warm baths—it is insufficient to correct deficiencies or meet daily requirements.
Topical minerals can serve as a supportive measure but should not be relied on as a primary source. Adequate dietary intake and properly formulated oral supplements remain essential for maintaining systemic mineral balance.
Q. How do food sensitivities or allergies impact the choice of mineral supplements?+
Food sensitivities and allergies can restrict access to mineral-rich foods and influence the type of supplements needed.
For example, individuals with dairy allergies may have limited dietary calcium intake and require alternative sources. Similarly, those avoiding gluten, soy, shellfish, or corn need to avoid supplements that contain derivatives or excipients from those sources.
Many mineral supplements include fillers, binders, or flavoring agents that may trigger adverse reactions in sensitive individuals. Choosing hypoallergenic, vegan, gluten-free, or allergen-free formulations (like all ours) is essential in these cases.
In addition, food sensitivities that affect the gastrointestinal tract, such as celiac disease or inflammatory bowel conditions, impair mineral absorption. This situation may require adjusted dosing to maintain adequate status.
Q. Are there specific minerals important for cognitive or mood health that aren’t well known?+
Yes. In addition to widely recognized minerals like magnesium and zinc, several lesser-known minerals and trace elements contribute to brain function and mood regulation:
Boron supports cognitive performance, memory, and neuronal signaling essential for normal brain function.
Selenium contributes to antioxidant defenses in the brain and regulates thyroid hormones essential for neurological stability.
Copper is required for neurotransmitter synthesis, myelination, and overall brain development.
Manganese supports mitochondrial function and serves as a cofactor for antioxidant enzymes that protect neural tissue.
Chloride maintains electrical excitability in neurons, regulates synaptic inhibition through GABA signaling, and helps control brain pH and osmotic balance.
Iodine is essential for the synthesis of thyroid hormones, which regulate brain development, energy metabolism, and cognitive performance. Even mild deficiency in adults can impair attention, memory, and processing speed. Iodine deficiency during pregnancy and early childhood can cause irreversible neurodevelopmental damage, including cretinism. Adequate intake is critical during gestation and lactation to support fetal and infant brain development.
Other mineral deficiencies that cause fatigue, poor sleep, unstable blood sugar, or symptoms of ADHD can also impair cognition, focus, and memory. These indirect effects are common but often misattributed to other causes.
Q. How do environmental exposures to heavy metals and pollutants impact mineral needs or risks?+
Exposure to heavy metals such as lead, mercury, cadmium, and arsenic can disrupt mineral balance by competing with essential minerals for absorption, transport, and enzyme binding sites. For example, lead and cadmium interfere with calcium and zinc metabolism, increasing the risk of deficiency and impairing related physiological functions.
Prolonged exposure can deplete mineral reserves, impair enzyme activity, and exacerbate toxic effects. Maintaining adequate mineral status is essential for metabolic resilience and protection against environmental toxicants.
Environmental pollutants disrupt structural metabolism and enzyme regulation, increasing the body's demand for minerals involved in detoxification, cellular repair, and tissue integrity. Minerals such as selenium, zinc, and copper are required for the synthesis and function of key detoxification enzymes, including those that regulate sulfur metabolism, protein folding, and metal transport. Chronic exposure increases turnover of these minerals and may deplete reserves critical for maintaining metabolic stability.
Q. Are there differences in mineral needs for people living in different climates or altitudes?+
Yes. Climate and altitude can affect mineral requirements through changes in metabolism, fluid loss, and environmental exposure.
At high altitudes, lower oxygen availability alters energy metabolism and increases the turnover of minerals involved in mitochondrial function and red blood cell production—such as iron, copper, and magnesium. Cold environments may increase caloric needs and elevate urinary and respiratory mineral losses, especially for calcium, potassium, and magnesium.
In hot or humid climates, heavy sweating leads to greater losses of sodium, potassium, magnesium, and chloride, which must be replaced to maintain fluid balance and neuromuscular function.
Regional soil composition and local dietary habits also affect baseline mineral intake, potentially compounding or mitigating climate-related demands. Mineral supplementation may be necessary when local food sources or environmental conditions create consistent deficits.
Takeaways
The takeaways below summarize the core insights on mineral nutrition and deficiency covered throughout the article:
Mineral deficiencies are often subtle and under-recognized but have a widespread impact. Many minerals beyond the common ones like calcium and magnesium are rarely discussed, yet they play essential roles in metabolic, neurological, and skeletal health. Their insufficiency can contribute to chronic diseases, cognitive decline, and impaired immune function.
Diet and water quality profoundly influence mineral status. Pristine water sources rich in minerals support optimal mineral intake, while treated or filtered municipal water commonly lacks essential minerals, potentially exacerbating deficiency risks if not compensated by diet or supplements.
Individual factors such as age, lifestyle, medications, and genetics alter mineral needs. Mineral requirements vary with physiological conditions like pregnancy, menopause, aging, physical activity, gut health, and genetic polymorphisms, emphasizing the need for personalized nutritional assessment and supplementation.
Common medications and dietary patterns affect mineral balance. Drugs like antacids, diuretics, and antibiotics, as well as popular diets (keto, vegan, intermittent fasting), can impair mineral absorption or increase losses, necessitating adequate monitoring and tailored supplementation strategies.
Mineral interactions are complex and require mindful supplementation. Some minerals compete for absorption, and high doses of one may impair another's uptake; spacing intake and choosing balanced formulations improve bioavailability and prevent adverse effects.
Professional-grade supplements often use highly bioavailable mineral forms. Whether “natural” or synthetic, the key to effective supplementation lies in mineral form, quality, and bioavailability; formulations that mimic natural complexes and chelated minerals tend to offer better absorption and tolerability.
Environmental toxins increase mineral demands and risks. Exposure to heavy metals and pollutants disrupts mineral metabolism, depleting antioxidant minerals and increasing the need for adequate mineral nutrition to support detoxification and resilience.
Early detection of mineral deficiencies is possible and important. Laboratory tests beyond routine blood work—including urine, red blood cell analysis, and combined clinical assessment—can identify hidden deficiencies before symptoms become overt, allowing timely intervention.
Public health measures like iodized salt are critical but face challenges. While iodization has dramatically reduced iodine deficiency, widespread anti-salt messaging reduces overall salt intake, risking inadequate iodine consumption that may contribute to rising neurodevelopmental disorders.
Holistic approaches considering diet, lifestyle, environment, and individual variability ensure optimal mineral health. Addressing mineral sufficiency requires an integrative perspective that includes quality nutrition, mindful supplementation, water quality, and environmental factors for lifelong wellness.
Recognizing and addressing mineral deficiencies is a critical but frequently underappreciated foundation of long-term health maintenance. Through informed dietary choices, quality supplementation, and awareness of individual and environmental influences, you can better prevent and manage subtle deficiencies before they turn into chronic illness and cognitive decline.
Author's Note
I was blessed to be born in Lviv, Ukraine, a gorgeous medieval city in the foothills of the Carpathian Mountains. Thanks to its unique geography, our town’s water wasn’t drawn from nearby rivers and lakes but pumped directly from pure, mineral-rich mountain springs.
This spring water was pristine, abundant, unprocessed, and supplied our community with a full range of essential minerals and trace elements, except for iodine, which was notoriously low in our region.
Endemic (regionally limited) iodine deficiency led to a widespread public health prevention practice: all children, from kindergarten through high school, were regularly supplemented with iodine lozenges. Each week, we would line up as a group, and a nurse would place a sweet lozenge into every child’s mouth.
This routine was taken very seriously to prevent the cognitive and developmental challenges associated with iodine deficiency, given the known risk in our region. Mind you, we’re talking about the post–World War II Soviet Union in the 1950s and 1960s, not the current “era of enlightenment” in the prosperous United States.
Decades later, when I began counseling Russian- and Ukrainian-American clients in Brooklyn, New York, home to one of the largest immigrant communities from the former Soviet Union, I noticed an interesting pattern. Most of my clients were from major cities like Kyiv, Moscow, and Saint Petersburg (Leningrad), whose drinking water came from large rivers. These cities were known for having soft and heavily processed water, with little to no minerals and trace elements. Not surprisingly, I can count clients from Lviv on one hand among the several thousand I counseled from other regions.
My personal experience illustrates how local water and the good luck of being born in the right place can affect lifelong health in ways that are not immediately obvious but have long-term implications.
Today, most municipal water systems rely on rivers, lakes, or rain-collecting reservoirs. These sources can become easily polluted by industrial waste, farm chemicals, or the breakdown of old pipes and infrastructure. The ensuing water treatment processes result in soft water that lacks minerals and trace elements. This situation is compounded by many people relying on bottled or filtered water, which strips even more minerals.
Without adequate compensation with supplements, these mineral gaps may negatively impact long-term health—particularly cardiovascular and brain function, bone density, dental health, and the neurological system.
To conclude, regardless of where you were born or live now, don’t get screwed by counting on your luck alone!
***
If this free article gave you insight into a topic rarely covered by mainstream medical media objectively and in similar depth, that’s no accident. I work independently and have no financial ties to pharmaceutical companies, hospitals, or institutional sponsors.
That independence allows me to present the facts without having to serve anyone’s agenda. If you find this approach valuable for your well-being, the best way to support my work is by sharing this article with others.
Every repost, forward, or mention helps amplify the reach and makes future work like this possible. Thank you for taking the time to read and for supporting my work!