
How to Lower Blood Sugar Without Fail
If you have already tried and failed to normalize high blood sugar and recover from metabolic syndrome, prediabetes, or type 2 diabetes, it was meant to be that way, because their treatment in the United States is focused on keeping you coming back for more blood tests and prescriptions rather than on your recovery.
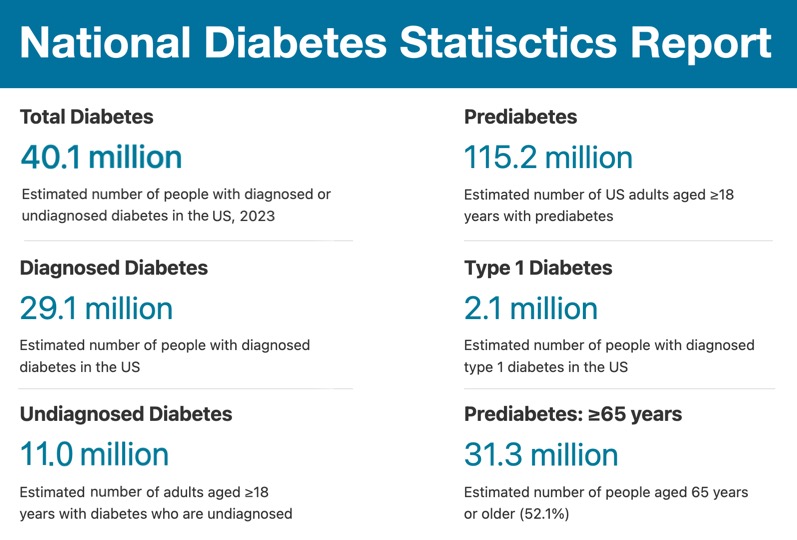
And you are certainly not alone. Here are the most recent numbers for patients with high blood sugar-related disorders from the 2023 statistics report (most recent available) by the United States Centers for Disease Control and Prevention [link]:
This guide explains what happens during treatment, starting with the condition known as "insulin resistance."
For almost a century, insulin resistance has shaped how medical professionals and drug companies explain and treat high blood sugar, prediabetes, and type 2 diabetes. It sounds scientific, but in fact, it is a sham because insulin resistance is physiologically impossible.
In reality, high blood sugar and, by extension, diabetes and prediabetes are not caused by resistance to insulin but by your body's inability to utilize excess glucose fast enough.
This guide also explains why treating high blood sugar with more insulin or insulin-stimulating drugs makes the patient worse while making the lab report look better.
The Origins of the Insulin Resistance Theory
The term "insulin resistance" was first introduced by Dr. Wilhelm Falta, a Czech physician, in 1931. He proposed this condition as the underlying cause of type 2 diabetes [link].
It was later promoted in the United States by the late Dr. Gerald Reaven, an endocrinologist and professor emeritus of medicine at Stanford University School of Medicine, who is considered the "Father of Insulin Resistance" [link].
The "insulin resistance" concept is seemingly self-explanatory:
Insulin is a hormone produced by the pancreas that, among other functions, regulates glucose levels in the blood, commonly known as "blood sugar."
When glucose levels rise after meals containing carbohydrates, the pancreas secretes insulin to help cells use glucose for immediate energy or store it for future use as glycogen in the liver and muscles or as fat in adipose tissue.
Thanks to insulin, blood sugar goes down in healthy people and does not cause the disorders and side effects associated with elevated blood glucose.
However, in some people with a normally functioning pancreas, insulin and blood sugar levels remain stubbornly high, a condition known as either prediabetes or type 2 diabetes.
Based on the description above, it is not difficult to apply deductive logic to this situation. Deductive logic is a method of reasoning in which conclusions are drawn from general premises. If the premises are true, the conclusion must also be true.
Here is a simple example of deductive reasoning: "If it is dark outside and the time is 8 p.m., then it is night."
In the case of high insulin and high blood sugar, the reasoning was, "If insulin and blood sugar levels are both high, then the cells that are supposed to utilize glucose must be resisting insulin's signal to do so. Hence, the person with this condition is 'insulin resistant.'
And try arguing against this logic when it is promoted by a professor of medicine at Stanford University, endorsed by the American Diabetes Association, written up in medical journals and medical references, and taught in medical schools and mandatory continuing education courses for medical professionals.
Here, for example, is an excerpt from the Merck Manual of Diagnosis and Therapy, Professional Edition [link]:
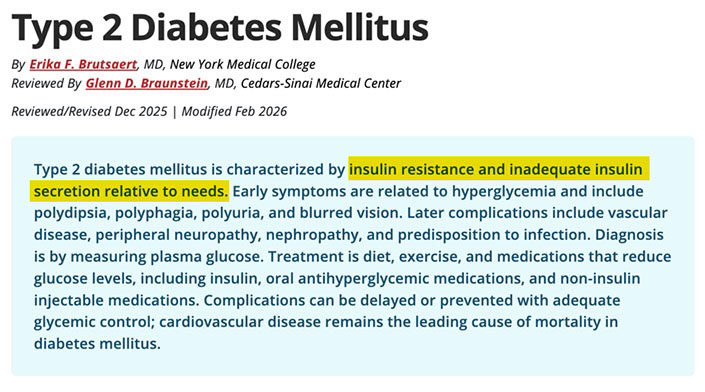
This recent article mentions "insulin resistance" 12 times, and the term appears dozens more times in other articles related to diabetes and metabolic syndrome.
But is any of it true?
No, it isn't, and here is why, in simple terms...
Why "Insulin Resistance" Isn't Possible
Under average daily load, meaning a mixed diet and moderate activity, the average glucose utilization rate is approximately 8 to 10 grams per hour when averaged over 24 hours, or 190 to 240 grams daily.
The brain consumes about 50% of that amount, or up to 120 grams daily. Red blood cells, the liver, and the kidneys use another 60 to 80 grams daily. During exercise or hard labor, muscles can increase glucose consumption 10 to 40 times.
So what happens if you consume more than 240 grams of carbohydrates and are not involved in hard labor or intensive exercise?
Glycogen is the primary storage pathway for excess glucose. The liver stores about 100 to 120 grams, and muscles store 300 to 500 grams, but only to the extent that those stores have been utilized. The conversion of glucose to fat is limited, usually less than 5% of excess glucose.
So unless fasting, physical work, or exercise has created room in liver and muscle glycogen stores, excess dietary glucose has nowhere easy to go. When glucose enters the bloodstream faster than the body can use or store it, it does not disappear because more insulin is present. It remains elevated longer and is registered on a blood test as "high blood sugar."
After a carbohydrate-containing meal, glucose enters the bloodstream, and the pancreas responds by releasing insulin. Under normal conditions, insulin helps move glucose into muscle and fat cells and tells the liver to stop releasing its own glucose into the blood.
When this system works properly, blood glucose rises after a meal, insulin rises in response, tissues take up glucose, the liver slows glucose output, and blood sugar gradually returns to baseline.
The problem begins when the amount of glucose entering the bloodstream repeatedly exceeds the body's ability to utilize it, and the pancreas compensates by producing more insulin.
That is how a person can have both high insulin and high blood sugar at the same time. The pancreas is still trying to compensate, but the liver, muscles, fat cells, and other tissues are no longer responding to insulin effectively.
To summarize, high blood sugar appears not because insulin is absent, insufficient, or "resistant," but because your body can no longer utilize excess glucose fast enough.
What I just described is Medical Biochemistry 101 and has been widely taught in medical schools worldwide for at least a century, ever since Dr. Frederick Banting isolated insulin in 1921, treated the first patient with it in 1922, and received the Nobel Prize in Medicine for his discovery in 1923.
Despite all of that, the American Diabetes Association, the mouthpiece of the diabetes care industry, claimed as recently as 2023 that the cause of "insulin resistance" is still a mystery:
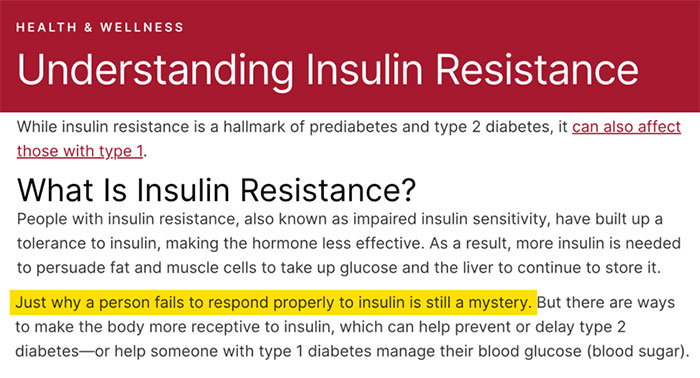
In other words, the term "insulin resistance" is a sham based entirely on a "mystery," and a perfect vehicle for pushing injectable insulin and insulin-stimulating drugs to create the illusion of better "blood sugar control."
How Patients Pay for the "Insulin Resistance" Sham With Their Health and Lives
It would not be a big deal if not for one thing: excessive insulin is not harmless. When blood sugar is lowered by forcing more insulin into an already overloaded system, excessive insulin becomes one of the central drivers behind the most deadly complications of type 1 and type 2 diabetes, ranging from high blood pressure, heart attacks, and strokes to kidney failure and limb amputations. Let me explain:
Injectable insulin for type 1 diabetes. External insulin keeps type 1 diabetics alive. That doesn't make excessive insulin harmless. When insulin is repeatedly used to cover excessive carbohydrate intake, glucose readings may look better, but the price is higher insulin exposure, weight gain, fluid retention, more hypoglycemia, and the endless cycle of eating to correct insulin lows, then taking more insulin to correct the resulting highs. 2.1 million Americans are affected by this condition.
Insulin-stimulating medications for type 2 diabetes. Drugs that force the pancreas to produce more insulin can make blood sugar look better while pushing the same overloaded system even harder. The patient may get a lower glucose reading, but the price can be higher insulin exposure, weight gain, hypoglycemia, hunger, and faster beta-cell exhaustion. 40.1 million Americans are affected by this condition, 11 million of them undiagnosed.
Weight gain. Insulin is a fat storage hormone. In excess, it stimulates fat storage and makes stored fat harder to lose. The heavier the patient gets, the more insulin is often required, and the more insulin is used, the easier it becomes to gain still more weight. 170 million-plus Americans (72.4% of the population) are overweight or obese.
Prediabetes. According to the American Diabetes Association (ADA), prediabetes is defined as blood glucose levels that are higher than normal but not yet high enough to be diagnosed as diabetes. Elevated insulin (hyperinsulinemia) is the defining characteristic of the prediabetes underlying mechanism. This condition affects a staggering 115.2 million Americans over 18 years old.
High blood pressure. Excess insulin promotes fluid retention and vasoconstriction, or narrowing of the blood vessels. The glucose number may look better, but the vascular system pays for it through a squeeze-bottle effect: more fluid inside tighter blood vessels. With better-looking glucose numbers, the patient may be told that blood sugar is "better controlled" while blood pressure, swelling, and cardiovascular risk are getting worse. Hypertension affects nearly half of U.S. adults, about 120 million people. Among adults 60 and older, over 70% are affected.
Heart attacks and strokes. Chronically high insulin promotes inflammation, endothelial dysfunction, elevated triglycerides, vascular smooth muscle changes, and atherosclerosis. A better glucose number obtained by forcing more insulin into the system may improve the lab report while worsening the vascular disease that kills the patient. Heart attacks and strokes kill over 500,000 Americans each year. In 2023, cardiovascular disease caused 919,032 deaths, or roughly 1 in every 3 deaths.
Kidney disease. As with heart disease, excess insulin increases sodium retention, fluid retention, blood pressure, and vascular strain. Over time, these conditions accelerate kidney damage and can eventually lead to kidney failure. About 37 million American adults have chronic kidney disease, or roughly 1 in 7. More than half a million Americans are on dialysis. Most patients with CKD die from cardiovascular and other related causes before kidney disease itself is listed as the direct cause of death, so the annual death count attributed specifically to kidney disease appears lower than the true burden, at just over 50,000.
Limb amputations usually occur after years of vascular disease, nerve damage, poor wound healing, infection, and impaired blood flow, all intensified by insulin's vasoconstrictive and inflammatory effects on the delicate blood vessels of the extremities. The American Diabetes Association reports that about 160,000 people with diabetes undergo amputation each year in the United States. Over a decade, that means roughly 1.5 million diabetes-related amputation events.
Liver disease. Insulin directs the liver to store glucose as glycogen and convert excess glucose into fat when glycogen capacity is reached. According to the American Liver Foundation, non-alcoholic fatty liver disease affects an estimated 80 to 100 million Americans. It can progress from simple fat accumulation to liver inflammation, scarring, cirrhosis, liver failure, and liver cancer. Once cirrhosis develops, the liver can no longer reliably handle detoxification, protein production, bile flow, glucose regulation, and blood-flow control. As with kidney disease, many people die from cardiovascular and other metabolic complications before non-alcoholic liver failure is listed as the direct cause of death.
Dementia and cognitive decline. Excess insulin is tied directly to brain aging through vascular injury and inflammation. In insulin-treated patients, the immediate brain danger is severe hypoglycemia that can push glucose below the brain's operating range. It can cause confusion, falls, seizures, coma, heart rhythm disturbances, and sudden death.
The brain does not use insulin the same way muscles, kidneys, or the liver do, but abnormal insulin exposure still affects memory and brain health. When treatment lowers blood sugar by driving insulin higher, the glucose number may improve while the brain continues to age faster. An estimated 7.2 million Americans age 65 and older are living with Alzheimer's dementia, and Alzheimer's disease caused 116,022 deaths in the United States in 2024.
The Side Effects of Treating "Insulin Resistance" With More Insulin
The following conditions are also connected to elevated insulin. They may receive less attention than the major complications above, but they still add to the overall damage:
Gastroparesis. Gastroparesis makes insulin treatment dangerous because the drug acts on schedule while the stomach empties unpredictably. Insulin may peak before food reaches the intestine, causing hypoglycemia, followed later by hyperglycemia when the delayed meal is finally absorbed. The patient is then forced into another cycle of sugar correction and insulin correction.
Blindness and diabetic retinopathy. The retina is damaged by abnormal glucose metabolism, high blood pressure, inflammation, impaired blood flow, and small-vessel injury. Excess insulin can lower glucose readings while promoting weight gain, fluid retention, higher blood pressure, and continued metabolic overload. The eyes may still be deteriorating while the A1c looks better.
Hearing loss and tinnitus. Excess insulin worsens the same vascular and inflammatory conditions that injure the cochlea: high blood pressure, fluid retention, impaired microcirculation, weight gain, and continued metabolic overload. The inner ear is a small, high-demand organ. It does not tolerate years of vascular stress well.
Neuromuscular disorders. Excessive insulin keeps the body in storage mode, suppresses fat mobilization, promotes weight gain, and contributes to fluid and electrolyte shifts. Muscles and peripheral nerves become heavier, weaker, less efficient, and less tolerant of activity. The result is more fatigue, cramps, poor coordination, weakness, and functional decline.
Cancers. Excessive insulin promotes a pro-growth and pro-inflammatory internal environment. Insulin and related IGF signaling encourage cell proliferation, reduce normal cell death, and interact with inflammatory pathways that favor abnormal growth. Insulin alone does not explain cancer, but chronic hyperinsulinemia helps create conditions in which cancer can develop and progress.
Bone disorders. Excess insulin does not strengthen bones. It promotes weight gain, inactivity, fluid retention, and repeated metabolic instability. Once high blood sugar develops, frequent urination increases the loss of water and minerals. Over time, this combination weakens bone remodeling and contributes to osteoporosis, fractures, and, when vitamin D and mineral metabolism are disturbed, osteomalacia.
Insomnia. Excess insulin keeps the body metabolically activated and causes restless sleep, early waking, nighttime hunger, sweating, agitation, and the feeling of being tired but unable to settle.
Rage, irritability, and conflict-prone behavior. Insulin is not only a storage hormone. In evolutionary terms, it also helps direct incoming energy into action, recovery, and survival. When insulin remains excessive, the body may stay in an overactivated metabolic state instead of returning to baseline. That can show up as impatience, irritability, agitation, impulsive reactions, and conflict-prone behavior. The person may think he is reacting to other people, but the body is already primed for confrontation.
Polypharmacy. Once treatment focuses on forcing blood sugar lower instead of reducing the glucose and energy overload, one drug becomes several. Insulin or insulin-stimulating drugs are followed by blood pressure drugs, statins, diuretics, pain drugs, acid-suppressing drugs, and drugs to manage side effects from other drugs. "Diabetes management" turns into medication management.
Premature aging and reduced life expectancy. Excess insulin adds accumulated damage to all of the above conditions. Together they cause accelerated decline and premature aging. People with type 1 diabetes live longer today than they did in the past, but insulin treatment has not restored normal lifespan for many of them because of the long-term cardiovascular, renal, neurological, and metabolic damage that follows a lifetime of unstable blood sugar and excessive insulin exposure.
Scared? Amazed? Bewildered? Me too!
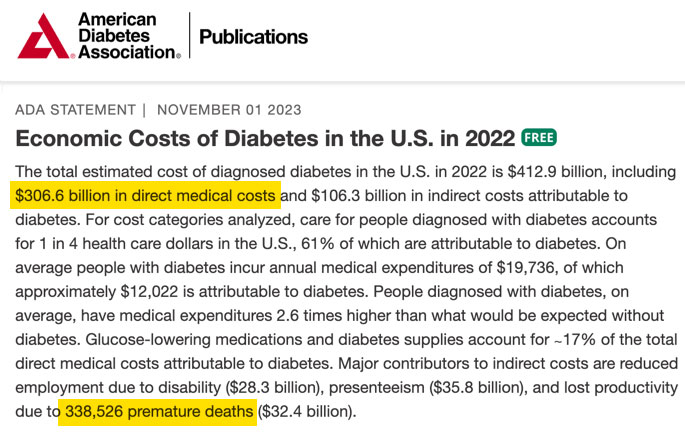
All of these complications are the price well over a hundred million Americans are paying with their health and lives for one seemingly innocent 'insulin resistance' term introduced in 1931 by Dr. Falta, reintroduced in 1988 by Dr. Reaven, and sustained to this day by the commercial interests behind the $300 billion-plus diabetes-care industry [link]:
So how do you get out of this trap? Let me repeat what I wrote at the beginning of this guide:
To summarize, high blood sugar appears not because insulin is absent, insufficient, or resistant, but because the body can no longer utilize excess glucose.
In other words, at a certain point, a normally functioning body can no longer process excessive dietary carbohydrates, no matter how much insulin the pancreas produces or how much insulin is delivered from an external source, such as an injection or pump.
IT IS NOT INSULIN RESISTANCE. What is measured as HIGH BLOOD SUGAR is glucose the body has not yet utilized, and the process will not speed up just because more insulin is present.
In plain language, if your pancreas is functioning normally but your blood sugar is high, ANYONE telling you a long story about INSULIN RESISTANCE is either an idiot, a fraudster, or both.
And, by the way, if your insulin level is CHRONICALLY HIGH, it means your pancreas is still doing its job well: producing insulin in response to elevated blood glucose, as it is supposed to.
Therefore, the idiot-proof treatment for "insulin resistance" is as simple as it gets: reduce the amount of carbohydrates in your diet to a level that does not exceed your body's needs!
After you do that, your blood sugar will gradually return to normal, and so will your insulin level, because the pancreas will not have to pump out insulin again and again to reduce glucose in the blood.
As simple as it gets. In my own case, recovery did not require doctors or drugs because the problem was excessive glucose load, not "insulin resistance" or any other sham factor. That is precisely how I recovered from my own encounter with undiagnosed late-stage type 2 diabetes 28 years ago, and I remain healthy to this day.
How to normalize blood sugar and eliminate a state known as "insulin resistance"
Here are several tips to make this process as smooth as possible:
Stop thinking of insulin resistance, type 2 diabetes, and prediabetes as permanent diseases because they aren't. They are functional metabolic disorders driven primarily by diet, lifestyle, and glucose overload. In medical literature, type 2 diabetes is described as a syndrome (a collection of symptoms), while prediabetes is defined as elevated blood glucose that has not yet crossed the diabetes threshold. That makes both conditions different from "organic" diseases, such as heart failure or cancer.
Recall the diet and lifestyle of your great-grandparents on both the maternal and paternal sides. As much as practicable, move closer to their dietary and lifestyle pattern to reduce your risk of modern Western diseases. There is a reason why most second- and third-generation immigrants to the United States from longevity regions, such as Japan, lose their longevity advantage after shifting to a Western diet and lifestyle.
Avoid foods your ancestors did not consume regularly. Your immune and endocrine systems may not tolerate them well, leading to allergies, inflammation, cravings, and excessive appetite that are nearly impossible to reverse without changing your diet composition.
Reduce the quantity and frequency of meals, and eliminate all snacks. This is the easiest way to eat less and reduce carbohydrate consumption. In my own case, I have been eating only twice a day for the past 30 years, and this helped reduce my appetite and strengthen my digestive health because the less food and less often my stomach and intestines had to digest, the less prone they became to inflammation and ulceration.
Avoid alcoholic beverages. Low-alcohol drinks, such as beer, ale, mead, cider, and kvass, were consumed for millennia partly because they were safer than contaminated raw water. But they were not distilled or concentrated to modern high-alcohol levels.
Alcohol is a no-no for anyone with high blood sugar and high insulin because it drives appetite, causes sugar cravings, reduces glucose utilization, and damages the liver's ability to regulate blood sugar.
In my own case, I replaced alcoholic beverages with non-alcoholic beers, but I avoid so-called IPA (Indian Pale Ale) beers because many of them are naturally sweet.
Eliminate anything that tastes sweet, naturally or artificially, because sweetness keeps the insulin-appetite-craving loop active even when little or no sugar is present. Without this step, normalizing blood sugar and reducing insulin secretion is nearly impossible.
I can now tolerate an occasional dessert, such as ice cream, but no more than 10 to 15 times per year. I realize this is difficult for most people because sweets and sweetness are as addictive as smoking or drinking, but making this effort beats taking medication, aging prematurely, or dying from diabetes-related complications.
If you eat fruits, vegetables, or berries with high sugar content, consume them only in moderation and only during their natural ripening seasons. This suggestion applies only to people who are still healthy but are concerned about future risk. The fact that strawberries or bananas are available year-round in the supermarket does not mean it is fine to eat strawberries in January or bananas every day, especially if you are already affected by metabolic syndrome, prediabetes, or diabetes.
Do not drink fruit juices or smoothies because they are loaded with sugar. A 240 ml, or 8 oz, glass of store-bought orange juice may contain 20 to 40 grams of sugar, equivalent to roughly 1.5 to almost 3 tablespoons of sugar.
Would you knowingly eat that much sugar by itself? No, you wouldn't. Incidentally, juices and smoothies are served ice-cold because cold blunts the taste of sweetness, making it easier to consume large amounts of sugar without discomfort.
Do not consume vegetable oils in large quantities, including highly prized olive oil. Humans need essential fatty acids, especially omega-6 and omega-3 essential fatty acids, but only in small amounts.
Olive oil is mostly oleic acid, a monounsaturated fat that the body can synthesize. It is not biologically essential in the same way as essential fatty acids and their long-chain derivatives, such as EPA and DHA from fish and seafood.
Concentrated oils are also easy to overconsume because they add a lot of calories without adding much bulk or enhancing satiety. They contribute to weight gain that, in turn, stimulates appetite for carbohydrates. That's the connection.
Take high-quality supplements daily to compensate for their deficiency in a moderate urban diet, the loss of nutrients in foods that are no longer eaten right after harvesting them, and the absence of mineral-rich natural water from mountain springs or deep wells.
Of all the factors listed above, a dollar's worth of supplements a day can make an enormous difference between malnutrition and sickness at 50 and remaining functional into your sixties, seventies, and beyond, as happened to me and my wife.
Supplements also reduce appetite and cravings driven by the body's response to vitamin and mineral deficiencies. Salt cravings are the most obvious example. Other common examples include cravings for chocolate when the body is short of magnesium, meat when it is short of iron, dairy when it needs protein or trace elements, and sour foods when it is short of minerals, amino acids, B vitamins, electrolytes, or other essential nutrients.
In my own case, I was able to recover from late-stage type 2 diabetes and remain in remission for almost 30 years, mostly thanks to taking professional-grade supplements during this time.
If I had followed all of the above recommendations without supplementation, I would have died a long time ago from malnutrition-related neurological, cardiovascular, or oncological complications.
-
Do everything gradually to prevent hypoglycemia, or very low blood sugar, which is far more dangerous than high blood sugar. The pancreas is conditioned to release insulin not only in response to what you eat but also in response to when you usually eat. This physiological response is called a conditioned reflex and has been well known since Pavlov's experiments with his dogs.
If you are already on medication, reduce insulin and insulin-stimulating drugs as your blood glucose improves, and do so under careful monitoring. This is essential for recovery and for preventing medication-driven hypoglycemia.
When a doctor gives you a prescription for a glucometer and tells you to measure blood sugar at recommended intervals, it is not mainly to evaluate high blood sugar, as most people believe, but to prevent low blood sugar, which is far more dangerous.
Unfortunately, when low blood sugar happens, most doctors recommend compensating for it with fast-acting carbohydrates because that is easier for them to manage than reducing the dose of the drugs you are taking.
I realize this sounds stupid, and it is. But this approach is far more profitable for Big Pharma, Big Ag, Big Insurance, and Big Hospital Medicine than helping you take fewer drugs or no drugs at all.
- Study my site as if your life depends on it. I wrote down almost everything I learned to help people who are in the same situation I was. My work isn't as prominent as it should be because it flies in the face of the commercial interests mentioned above. The same interests are also behind "insulin resistance" and pretty much every other disease-management trap that affects Americans of all ages.
Avoid extensive physical exercise until your blood sugar and insulin have normalized to reduce the risk of injury, hypoglycemic episodes, and excessive appetite.
Brisk walking and household chores are the best forms of exercise for anyone, but especially for people past fifty, because they are the safest and most accessible forms of exercise.
These 14 points are enough to start lowering your blood sugar and eliminating "insulin resistance" nonsense from your patient record. The earlier you start, the faster and better you will recover from a condition that the diabetes treatment industry has every reason to keep alive because it keeps patients on drugs, tests, and treatments for the rest of their lives.
I can assure you that I am absolutely not an "anti-doctor" kind of person. Unfortunately, the term "insulin resistance" was first proposed before 99% of practicing doctors and pharmacists were born, so all of them, myself included, were taught to think this way.
And I am not alone in thinking this way. If your doctor, nurse practitioner, dietitian, or nutritionist dismisses this guide and calls me "crazy," point him or her to this article by a respected professor of medicine and his peers in a peer-reviewed medical journal (Chockalingam A, Natarajan P, Thanikachalam P, Pandiyan R. Insulin Resistance: The Inconvenient Truth. Mo Med. 2021, Mar-Apr; 118(2):119-121. PMID: 33840852; PMCID: PMC8029630):
Dr. Anand Chockalingam, MD, the lead author of this article, is a professor in the Division of Cardiovascular Medicine at the University of Missouri-Columbia, Columbia, Missouri, and is affiliated with the Cardiology Section at the Harry S. Truman VA Medical Center in Columbia, Missouri.
As you can see, the conclusions of this distinguished author and his co-authors closely match my argument: in most people with type 2 diabetes, elevated insulin is the consequence of raised glucose load, not the cause of it. This article was published in 2021. I wrote the same for the first time back in 2001 in Disorders of Carbohydrate Metabolism, my second Russian-language book on this topic.
What supplements do I take?
I take professional-grade supplements made in the United States and recommended on my site. Their content is fully disclosed, and if you prefer to buy yours from Amazon or elsewhere, you can compare their composition with what is available there.
Keep in mind that the same composition does not guarantee the same quality because it is determined not only by the amounts listed on the label but also by the sources of the raw ingredients used in manufacturing. For this reason, I recommend only the supplements I take myself. And as a former pharmacist, I know more about supplement quality than most people.
Here is what I take:
-
High-quality multivitamins. Coenzymated Once Daily Multi contains all essential vitamins, minerals, and trace elements required for metabolic health and helps compensate for what is missing from a moderate urban diet. Taking this type of supplement regularly can have the greatest impact on your health and longevity, regardless of what you eat or any other similar factor.
Extra calcium, magnesium, and vitamin C. For the past 26 years, I have been taking the Hydro-CM formula to maintain regularity because my large intestine was severely compromised by the high-fiber vegan diet that led to my bout with diabetes. In addition to vitamin C, this non-addictive formula contains highly absorbable calcium and magnesium, which helped protect me from osteoporosis and osteomalacia.
-
Hydro-CM replacement. If you aren't using Hydro-CM for constipation, I recommend taking instead the Calcium-Magnesium and PureWay vitamin C formulas to supplement essential calcium, magnesium, and vitamin C.
-
Vitamin D-3. Although vitamin D-3 is included in the Once Daily Multi, I take an additional natural vitamin D-3 formula in a fat-soluble form. Vitamin D plays a significant role in structural metabolism, including cell growth, maintenance, and tissue remodeling throughout the body.
It also performs important protective roles in glucose metabolism, inflammation control, cell function, and neuromuscular function. These functions are especially important when the body is recovering from the damage caused by metabolic syndrome, prediabetes, and diabetes.
-
Natural Vitamin E. For the same reasons as with vitamin D-3, I take an additional Natural Vitamin E formula for its broad protective properties, especially after fifty. Vitamin E protects cell membranes from damage, which is particularly important when blood sugar, insulin, triglycerides, and inflammation are elevated.
It also supports vascular health, immune function, nerve function, and normal tissue repair. All of these factors are directly relevant to metabolic syndrome, prediabetes, diabetes, and the accelerated aging that follows long-term metabolic damage.
-
Cod Liver Oil. I take Liquid Cod Liver Oil daily, which we buy from Amazon. One teaspoon of cod liver oil contains about the same amount of omega-3 fatty acids as 10 capsules of fish oil, but it is less expensive and more effective.
-
Digestive enzymes. Many people with diabetes, and especially those with dental issues such as poor-fitting dentures or difficulty chewing, are affected by indigestion, delayed stomach emptying, and related gastrointestinal disorders. In those cases, I recommend our Gastrozymes formula, and almost everyone who takes it swears by it. I do not take it myself because my teeth are still healthy and my stomach functions normally.
There are many other supplements specifically recommended for people with diabetes and "insulin resistance," such as alpha-lipoic acid, coenzyme Q10, L-carnitine, berberine, cinnamon, and others. I do not take any of them because I prefer a more conservative and sustainable approach focused only on the essential basics listed above.
Author's note
"Konstantin, your article implies that doctors are stupid and you are smart. It just doesn't make any sense."
I don't blame you for thinking that way. It doesn't make any sense to me either.
And no, doctors aren't stupid, and I am not smarter than they are. I just do different work than they do. If I or my wife gets seriously sick, God forbid, we will see a specialist because, thank God, he or she wasn't spending the past 30 years writing books and guides about nutritional disorders but mastering their medical specialty.
If my recommendations don't satisfy you, ignore everything I wrote about insulin resistance and continue treating it, and everything else, under the guidance of your doctor. If you recover from diabetes and eliminate insulin resistance, please let me know so I can share this doctor's name with my readers.
And if not, it is never too late to try my suggestions.
***
If this free article gave you extra insights into a topic rarely covered by mainstream medical media objectively and in similar depth, that's no accident. I work independently and have no financial ties to pharmaceutical companies, hospitals, or institutional sponsors.
That independence allows me to present the facts without having to serve anyone's agenda. If you find this approach valuable for your well-being, the best way to support my work is by sharing this article with others.
Every repost, forward, or mention helps amplify the reach and makes future work like this possible. Thank you for taking the time to read and for supporting my work!