
How to overcome dependence on fiber and fiber-related constipation
Dietary fiber is literally a delayed-fuse mine inside your gut. This guide explains how to overcome unhealthy dependence on fiber without resorting to laxatives. It is essential for anyone who wants to reduce fiber consumption, and is especially useful for people who wish to lose weight or reverse diabetes.
Dietary fiber expands and transforms colorectal organs, and, eventually, causes a physical dependence similar to drug addiction. This unfortunate outcome is familiar to anyone who has failed a low-carb diet because of severe constipation.
The following colorectal and genitourinary disorders and conditions are commonly related to consumption of fiber with food or as laxatives:
Persistent flatulence; Abdominal bloating; Straining and irregularity; Dependence on laxatives to move the bowels; Hemorrhoidal disease; Chronic constipation; Sporadic diarrhea; Fecal incontinence; Irritable bowel syndrome; Diverticular disease; Anal fissures; Anal fistulas; Ulcerative colitis; Crohn‘s disease; Familial history of colon cancer; History of colorectal polyps; Premenstrual syndrome (PMS); Infertility; Spontaneous abortion of fetus; Polycystic Ovarian Syndrome (POS); Chronic fatigue syndrome; Diabetic nerve damage; Loss of control over the bowels; Anorexia; Megacolon; Rectocele, Appendicitis; Inguinal hernia; Fecal and urinal incontinence; Frequent urination; Urethral obstruction;
Practically all these conditions share several common characteristics — difficulties in moving the bowels, irregularity, and large or hard stools. To get well, you need to work backwards — first, reduce the fiber; second, normalize stools; and, third, restore normal bowel movements.
The first task is easy to do, but the second — normalizing stools — is an enigma. And the third depends on the second. So let‘s turn to Fiber Menace for guidance on what normal stools actually are:
Form Follows Dysfunction*Summing Up the Damages
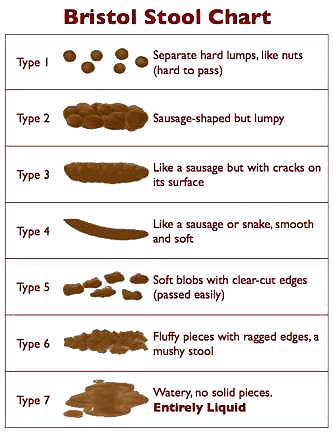
The British take their stools much more seriously than the Americans. Researchers at the Bristol Royal Infirmary—a hospital in Bristol, England—developed a visual guide for stools. This guide is called the Bristol Stool Form Scale, BSF scale for short. It is a self-diagnostic tool that helps skittish patients and doctors alike discuss this delicate subject without getting embarrassed.
Source: Wikipedia; licensed under the Creative Commons [link]
You just look at a simple chart, point to what approximates the content of your toilet bowl, and your doctor (or this book) tells you whether the form is right or wrong.
Type 1: Separate hard lumps, like nuts
Typical for acute dysbacteriosis. These stools lack a normal amorphous quality, because bacteria are missing and there is nothing to retain water. The lumps are hard and abrasive, the typical diameter ranges from 1 to 2 cm (0.4–0.8”), and they‘re painful to pass, because the lumps are hard and scratchy. There is a high likelihood of anorectal bleeding from mechanical laceration of the anal canal. Typical for post-antibiotic treatments and for people attempting fiber-free (low-carb) diets. Flatulence isn‘t likely, because fermentation of fiber isn‘t taking place.
Type 2: Sausage-like but lumpy
Represents a combination of Type 1 stools impacted into a single mass and lumped together by fiber components and some bacteria. Typical for organic constipation. The diameter is 3 to 4 cm (1.2–1.6”). This type is the most destructive by far because its size is near or exceeds the maximum opening of the anal canal‘s aperture (3.5 cm). It‘s bound to cause extreme straining during elimination, and most likely to cause anal canal laceration, hemorrhoidal prolapse, or diverticulosis. To attain this form, the stools must be in the colon for at least several weeks instead of the normal 72 hours. Anorectal pain, hemorrhoidal disease, anal fissures, withholding or delaying of defecation, and a history of chronic constipation are the most likely causes. Minor flatulence is probable. A person experiencing these stools is most likely to suffer from irritable bowel syndrome because of continuous pressure of large stools on the intestinal walls. The possibility of obstruction of the small intestine is high, because the large intestine is filled to capacity with stools. Adding supplemental fiber to expel these stools is dangerous, because the expanded fiber has no place to go, and may cause hernia, obstruction, or perforation of the small and large intestine alike.
Type 3: Like a sausage but with cracks in the surface
This form has all of the characteristics of Type 2 stools, but the transit time is faster, between one and two weeks. Typical for latent constipation. The diameter is 2 to 3.5 cm (0.8–1.4”). Irritable bowel syndrome is likely. Flatulence is minor, because of dysbacteriosis. The fact that it hasn‘t become as enlarged as Type 2 suggests that the defecations are regular. Straining is required. All of the adverse effects typical for Type 2 stools are likely for type 3, especially the rapid deterioration of hemorrhoidal disease.
Type 4: Like a sausage or snake, smooth and soft
This form is normal for someone defecating once daily. The diameter is 1 to 2 cm (0.4–0.8”). The larger diameter suggests a longer transit time or a large amount of dietary fiber in the diet.
Type 5: Soft blobs with clear-cut edges
I consider this form ideal. It is typical for a person who has stools twice or three times daily, after major meals. The diameter is 1 to 1.5 cm (0.4–0.6”).
Type 6: Fluffy pieces with ragged edges, a mushy stool
This form is close to the margins of comfort in several respects. First, it may be difficult to control the urge, especially when you don‘t have immediate access to a bathroom. Second, it is a rather messy affair to manage with toilet paper alone, unless you have access to a flexible shower or bidet. Otherwise, I consider it borderline normal. These kind of stools may suggest a slightly hyperactive colon (fast motility), excess dietary salt (sodium chloride), or sudden dehydration or spike in blood pressure related to stress (both cause the rapid release of water and sodium chloride from blood plasma into the intestinal cavity). It can also indicate a hypersensitive personality prone to stress, too many spices, drinking water with a high mineral content, or the use of osmotic (mineral salts) laxatives.
Type 7: Watery, no solid pieces
This, of course, is diarrhea, a subject outside the scope of this chapter with just one important and notable exception—so-called paradoxical diarrhea. It‘s typical for people (especially young children and infirm or convalescing adults) affected by fecal impaction—a condition that follows or accompanies type 1 stools. During paradoxical diarrhea the liquid contents of the small intestine (up to 1.5-2 liters/quarts daily) have no place to go but down, because the large intestine is stuffed with impacted stools throughout its entire length. Some water gets absorbed, the rest accumulates in the rectum. The reason this type of diarrhea is called paradoxical is not because its nature isn‘t known or understood, but because being severely constipated and experiencing diarrhea all at once, is, indeed, a paradoxical situation. Unfortunately, it‘s all too common.
*Excerpted from Fiber Menace, page 117-120;
BSF Chart: wikipedia.org
To avoid referencing non-descriptive numbers, I use the following definitions: types 1, 2 and 3 = hard or impacted stools. Type 4 and 5 = normal or optimal. Type 6 = loose stool, subnormal, or suboptimal, and type 7 = diarrhea.
In such cases as acute hemorrhoidal disease, anal fissure, or the inability to attain unassisted stools, loose stools (type 6) are acceptable. It‘s a messy experience, but which would you rather have — a bucketful of blood, pain, and an anal fissure that won‘t heal, or a brief lukewarm douche afterwards?
To restore and maintain normal stools (from type 4 to 6), the colon and rectum must first be free from hard and/or large stools (type 1 to 3). In our case, the opposite of hard isn‘t just soft, but also easy, small, and regular.
As you can see from the illustration (and, perhaps, already know firsthand from your own experience) “hard” stools can be “small,” “regular,” and “large.” Equally important, a “small” stool for one person can be “large” for another, because the perception of size isn‘t determined by a caliper, but by the aperture of one‘s anal canal. If the anal canal is constrained by enlarged internal hemorrhoids, even “small” stools, such as type 4, may be “difficult” to pass. Don‘t fall into this trap. The rule is: If stools are hard as in difficult, or not easy, or irregular, they are HARD, period!
Unless your stools are type 4 to 6 (normal), they are impacted. Impacted stools can be small, large, hard, soft, dry, moist—it doesn‘t matter. What “impacted” means is that they had a chance to pile up, compress, and dry out in the large intestine. Despite all of the nonsense you‘ve been hearing about “formed” stools, if yours are “very well formed,” most likely they are already impacted.
If we didn‘t have the Bristol Stool Form scale illustration in front of us, and you asked me what are normal stools, I would answer: normal stools are not noticeable during defecation!
Again, for someone with an intact anal canal, this may consist of formed stools as in type 4. For someone with hemorrhoidal disease, this may only be loose stools as in type 5 or 6. In other words, the normality differs from person to person, depending on the degree of prior damage. It‘s pretty much similar to defining pornography in the context of free speech: I can‘t tell you what pornography is, but I can tell when I see it. Similarly, I can‘t tell you what normal stools are, but you can tell when you don‘t have them yourself.
As you can see from the BSF scale, normal stools don‘t have to be round. After all, your anal canal isn‘t really round (when shut, it‘s actually flat), particularly if you already have enlarged internal hemorrhoids. So a flat shape is okay. In fact, when stools are already round as in type 4, it means you already have a slight degree of impaction. Otherwise their shape would be flattened up while passing through the anal canal.
Flat stools scare doctors a great deal because type 2, 3 and, to a lesser extent, type 4 may indicate the presence of a colorectal tumor. But that's because few doctors have ever observed normal (type 5) stools themselves.
Here is what's actually happening: think of the colon as a round mold. Then, it‘s easy to imagine why a tumor may change impacted stools from the round shape to a flat shape. This rare occurrence doesn‘t apply to type 5 stools, because their shape is formed primarily by the shape of the anal canal, not the colon‘s “mold.”
To rule out a tumor scare, just withhold your stools for few days to give them the opportunity to get molded. Observe their shape, and calm down yourself and your doctor. If you still worry, a tumor of the size capable of altering the shape of stools will show up instantly on abdominal x-ray with contrast medium — a much faster, cheaper, and safer alternative to colonoscopy in the case of severe hypochondria.
Let's summarize:
- Abnormal stools are any stools that require straining and/or you feel pressure from stools passing through the anal canal.
- Abnormal stools may be small or large size-wise, depending on fiber consumption, and frequency of defecation.
- Normal stools can be loose or slightly formed (Such as BSF type 5).
- Normal stools (between BSF type 4 and 6) aren‘t perfectly round.
- Normal stools for one person may be abnormal for another. The degree of normality is determined by the anatomy of the anal canal.
- Normal stools require zero effort and zero straining for elimination.
- Normal stools pass through the anal canal without any perception of pressure.
Of course, once you have damage to the anal canal, achieving absolute “normality” may not be easy. In this case you may have to accept a small degree of “abnormality” such as type 6 stools. This is no different from accepting gray hair, wrinkles, dental implants, and so on.
You may also have to live with the fact that after a certain degree of prior damage, caused by fiber, you won‘t be able to attain “unassisted” defecation and “normal” stools because of irreversible nerve damage, stretching of the large intestine, significantly enlarged hemorrhoids, and similar factors. I‘ll teach you how to overcome this problem as well without fiber and laxatives.
In fact, if I didn‘t know how to attain this seemingly impossible goal, I wouldn‘t be touching this subject or this site. I only got into this “game” when I was assured of having a winning hand. Otherwise, what is the point of maligning fiber if the only remedy is even more fiber.
Loosening up hard stools
Impacted stools (hard, type 1 to 3) and fecal impaction aren‘t the same. While stools are impacted, defecation is still attainable, even though it may be irregular or painful. Fecal impaction is a veritable medical emergency, because stools are no longer expelled no matter what.
Why am I getting into all these semantics? Well, these definitions are important. Some people, will, in fact, strain squeeze out their stools, and will say: “Oh, mine aren‘t hard?” and will keep straining, suffering, or taking me for a fool. And I don‘t want this outcome either for you or for myself. Others may say: “Oh, next to this idiot who didn‘t flush after himself/herself in the public bathroom, mine are small!”
Also, don‘t confuse the goal of having a colon “free from impacted stools” with the promise of or desire for a “clean” colon. The colon is never literally “clean” or empty because the transformation of liquid chyme into semi-soft stools is its job. Hence it always contains a certain volume (preferably small) of fecal matter, representing “work in progress.” Unlike the colon, the rectum indeed must be empty at all times, except during defecation.
A common suggestion to “cleanse” the large intestine with fiber or herbal laxatives is the worse form of quackery. Instead of helping, the herbal laxatives are actually contributing to constipation and colorectal damage because they irritate the intestinal mucosa, damage the nerve endings, kill intestinal bacteria, cause painful cramping, and may provoke severe diarrhea.
“Cleansing” with insoluble fiber, such as bran, is even more dangerous, because undigested fiber keeps piling up on top of already impacted, hardened stools. This may lead to obstruction, fecal impaction, and other complications, such as diverticular disease, megacolon, prolapsed hemorrhoids, or colon perforation — which is a mostly lethal condition.
The natural “cleansing” kits that provide a double- or triple punch—a combination of stimulant laxatives, such as senna; soluble fiber, such as psyllium husk; and insoluble fiber, such as bran—are the most dangerous. They may do the “trick” for someone with relatively intact and unobstructed colorectal organs, but someone with a longer history of constipation may end up in the ER either because of intense cramping caused by senna, or an allergic reaction to psyllium, or severe diarrhea from both, or impenetrable obstruction or colon perforation caused by bran, or combinations of all of the above.
In essence, sending triple-laxatives down into the dysfunctional colon is like blowing more and more helium into the balloon — it can only expand so much before it will blow up in your face.
The most common ways of loosening up and expelling hard stools rely on three methods: rectal enemas, water irrigation, and laxatives:
Rectal enemas stimulate vigorous colorectal peristalsis and invoke impossible to resist defecation. They are particularly effective for children who withhold stools, because their rectum and anus are exceptionally sensitive to external stimulation.
Disposable enemas, widely sold in pharmacies, are best used for this purpose. Just follow the instructions that accompany the product. Make sure to review contraindications, such as the symptoms of appendicitis, intestinal blockage, ulcerative colitis, heart disease, rectal bleeding, high blood pressure, kidney disease, and others.
Rectal enemas are marginally or not effective at all for people with chronic constipation, because the fluid doesn‘t reliably penetrate beyond the rectal cavity, and can‘t loosen up hard stools above the rectum. With some skill enemas can be used to lavage (wash out) the rectal cavity of hardened stools. Once the rectum is thoroughly lavaged, the stools accumulated in the sigmoid and descending colons are likely to move down and get expelled as well because fluids stimulate peristalsis.
Large volume enemas, delivered from a enema bag (douche bag), are difficult to administer without experience, and aren‘t likely to be effective for most people. Even if you can manage to deliver an enema solution past the rectum, few people can retain fluids long enough for it to be effective. If it “works,” it does it for the same reasons as a rectal enema, but with a lot more hassle and risk.
Water irrigation (also known as colon hydrotherapy or colonics) is more effective than enemas, though it too is limited to the rectum, sigmoid and descending colons. Water irrigation requires licensed facilities, a great deal of expertise, and the operator‘s integrity.
A special nozzle is inserted into the patient's anus and slowly advanced past the rectum and deep inside the colon. The nozzle is connected to two plastic tubes. One tube is attached to the water pump, which injects pressurized lukewarm water inside the large intestine. A vacuum pump removes the injected water and loosened-up fecal matter in the opposite direction, through the second tube.
Irrigation may induce cramping, and may not be very comfortable for some people. As with any invasive procedure, there are always risks of infection or colon perforation, because there is no visual control of the advancing nozzle. Water irrigation used to be quite popular in the first half of the past century, but eventually became controversial because of the exaggerated claims made by some of its promoters.
A less invasive form of colonic therapy is practiced the United States today. Here is how Ms. Pamela Gerry, a Registered Nurse and Certified Colonics Therapist (CCT) based in Springvale, Main [link] described it to me:
“Every therapist I know inserts a speculum only 1 inch into the rectum. There is nothing inserted deep within the colon, and the "nozzle" is not advancing. Most of the units in North America work on gravity flow in and out, and some use 1 psi infusion pressure, but no suction on the outflow.
Studies indicate colonoscopy is statistically much more likely to cause perforation that colonic irrigation. Most practitioners keep the water pressure under 1psi, but the safe limit allows an upper value of 2psi. I personally believe colonic hydrotherapy (CHT) is a very safe procedure. In 7 years I have not seen any perforation nor infection.”
This “soft” protocol may not be as quick and thorough at going inside the colon the old fashioned way, but, indeed, it must be quite safe, particularly in the caring hands of someone as considerate and experienced as Ms. Gerry. It is especially a good "first try" approach to resolve fecal impaction in young children and seniors before attempting a manual disimpaction in the hospital settings.
Laxatives are a non-invasive preparation, taken via the mouth. There are several types of laxatives, classified by their mechanism of action. The selection of a particular type is made based on a patient‘s age, health, contraindications, and degree of constipation. Most laxatives are addictive (i.e. cause dependence), and aren‘t intended for long-term use.
The right laxative—non-addictive, without side effects, and without a negative impact on digestion—is certainly the safest non-invasive method of loosening up hard stools and maintaining regularity in people who already have nerve damage (lack of urge), enlarged hemorrhoids (reduced aperture of anal canal), or who can‘t move the bowels unassisted because of age, infirmity, or trauma.
Unfortunately, there is no such a thing as a 'good laxative.' Here‘s a concise overview of various laxatives, presented by their mechanism of action:
These include fiber from natural sources, such as psyllium (Metamucil) or bran, and synthetic bulking agents, such as calcium polycarbophil (FiberCon) or methylcellulose (Citrucel).
Problems: Bulk-forming laxatives should not be used to normalize stools under any circumstances, because they may cause even more severe constipation or fecal impaction.
Conclusion: Not appropriate for the task of loosening up hard stools. Shouldn‘t be used for any form of constipation, because, just as with dietary fiber, bulk-forming laxatives can cause irreversible colorectal damage, as documented throughout this book.
Mineral oil (or its emulsion) passes through the small intestine unchanged. It lubricates (coats) hardened stools and, presumably, eases the passing of large stools.
Problems: Mineral oil does not break apart hard stools; it doesn‘t prevent the colorectal damage that can come from stretching and pressure; it doesn‘t alleviate straining. While transiting through the small intestine, mineral oil absorbs the fat-soluble vitamins A, D, K, and E. This “oversight” causes an acute deficiency of these vitamins—an especially troubling problem during pregnancy. Mineral oil may cause lipid pneumonia, if a small amount enters the lungs (a common occurrence among young children and impaired adults, who have problems with swallowing).
Conclusion: Useless at best, harmful at worse.
Emollient laxatives (stool softeners):
These are supposed to break down and soften hard stools, and are recommended for long-term use. Emollient laxatives are quite popular at hospitals and nursing homes. They are based on a synthetic compound called docusate, and sold under different brand names, such as Colace, Dialose, Diocto, DOS, Dosaflex, Genosoft, and others.
Problems: Docusate causes a depletion of potassium and magnesium, which in turn may cause muscular dysfunction and heart problems, particularly if enough potassium and magnesium isn‘t taken with a diet.
Since all cellular membranes are made of fat, emollients damage and penetrate the intestinal wall, enter the bloodstream, and are potentially carcinogenic.
Emollients permit the absorption of mineral oils and undesirable trans fats, which accumulate in the lymph nodes and can cause inflammation there. Docusate should not be used in combination with mineral oils. Emollients are slow acting and may take a week or more to act.
Conclusion: Unsuitable for long-term use, especially for older adults. Marginally effective for most people.
These are, essentially, diarrhea-causing agents, because they do not absorb in either the small or large intestine, and cause water retention. Lactose (milk sugar) and sugar alcohols, such as sorbitol, are “natural” hyperosmolar laxatives. Under the deceptive name of lactulose, lactose is sold as Kristalose, Cephulac, Chronulac, Cholac, Constulose, Enulose, and others. Polyethylene glycol (MiraLax, Polyethylene Glycol 3350) is a factory-made organic compound that acts just like lactose sans fermentation.
Problems: Lactose-derived hyperosmolar laxatives are unsuitable for people who are lactose-sensitive, because even a slight overdose may causes severe diarrhea. The fermentation of lactose inside the intestines causes bloating and cramping from gases produced by bacteria.
Polyethylene glycol-based laxatives damage bacterial flora, block absorption of nutrients throughout the GI tract, cause dependence, and, soon, intensify all of the symptoms of dysbacteriosis and constipation. They are especially problematic if you are already affected by hemorrhoids and/or fissures-related bleeding, since dysbacteriosis causes acute deficiency of vitamin K, and, correspondingly, clotting and healing problems, blood loss, anemia, and so on.
Conclusion: Ill-suited for many people, especially those who already suffer from intestinal disorders such as IBS, ulcerative colitis, and Crohn‘s disease. Life-long dependence and no chance of recovery. May cause acute dysbacteriosis, malnutrition, blood loss, chronic (pernicious) anemia.
These preparations cause inflammation of the intestinal mucosa and overstimulate the nervous receptors. The inflammation blocks water absorption, while the stimulation of the nervous receptors speeds up intestinal peristalsis. The best-known stimulant laxatives are castor oil (cascara is the active agent), senna (Ex-Lax, Senokot), bisacodyl (Dulcolax, Correctol), and aloe juice.
Problems: Stimulant laxatives are certainly “effective,” but at a cost—diarrhea, dehydration, loss of electrolytes (particularly sodium chloride), intestinal cramping, and decimation of normal intestinal flora — all of the side effects similar to ulcerative colitis and Crohn‘s disease.
Conclusion: Just like hyperosmolar laxatives, stimulants are unsuitable for anyone who is already suffering from intestinal disorders such as IBS, ulcerative colitis, or Crohn‘s disease, and are of dubious value for everybody else.
To stabilize rapidly rising osmotic or hydraulic pressure, the blood promptly ejects excess plasma and electrolytes (the ions of mineral or organic salts) into the colon. The ensuing surge of fluids inside the colon breaks down hard stools, and stimulates defecation by flowing down and filling up the rectum.
Two of the best known saline laxatives are Milk of Magnesia and Epsom Salts. Milk of Magnesia is an 8% water solution of magnesium hydroxide, Mg(OH)2. It has strong antacid properties, and interferes with gastric digestion if taken with food. Individuals with impaired kidneys may develop toxic levels of magnesium from extended use of Milk of Magnesia.
Epsom Salts is a brand name for magnesium sulfate. It‘s more potent than Milk of Magnesia because it absorbs faster, and may cause severe diarrhea, if overdosed. The risks in each are similar.
Problems. Indigestion when taken with food, abnormal kidney accumulation, possibility of diarrhea, dehydration, and a loss of sodium chloride (salt).
Conclusion: If used properly, osmotic laxatives are may be used for loosening up hardened stools or relieving occasional constipation.
It‘s apparent from the above overview that an osmotic agent would be the optimal tool to normalize stools, especially for people with nerve damage, anorectal disorders, and chronic constipation. Fortunately, I've developed such a “better agent.” Unlike Milk of Magnesia or Epsom Salts, it doesn‘t have any side effects and is suitable for long-term use.
Hydro-CM program
Originally, I developed Hydro-CM program for myself in order to get off laxatives and fiber. I had to overcome irritable bowel syndrome, chronic constipation, severe hemorrhoidal disease, anal fissures, and bleeding caused by a high-fiber vegetarian diet.
Before the Hydro-CM program, practically all trips to the bathroom were a torturous, dreadful experience, particularly without a laxative. I was trying to avoid laxatives because their residual side effects included an exacerbating round-the-clock pain and discomfort related to irritable bowel syndrome.
— Okay, okay, I'll have more fiber tomorrow!
I haven‘t had a single case of bleeding or acute hemorrhoidal disease since I began taking the Hydro-CM program regularly in 2000. It also erased a profound, paralyzing fear of going to the bathroom due to excruciating pain and a toilet bowl full of blood.
Similar outcomes have been confirmed by practically everyone who started with and continue using the Hydro-CM program after reading my books or following my recommendations. Also, since then, I am not as dependant on the Hydro-CM program because it has helped me to restore anorectal sensitivity and a natural urge. Obviously, I am free from IBS as well.
For those and many other good reasons I recommend using the Hydro-CM program to normalize stools and maintain regularity over other methods. Please review the Hydro-CM program page for additional detailed information about its content, application, benefits, safety, indications, frequently asked questions, and related facts.
— Try a corkscrew, dear!
If it upsets you that I can‘t provide a one-page “quick fix” to eliminate fiber dependence, constipation, and other colorectal problems that you may have accumulated over prior 10-20-30 or more years, don't get upset — sleight of hand isn't my specialty.
Michael R. Bloomberg, a self-made billionaire and extraordinary successful mayor of New York, put it this way in a recent radio broadcast:
“If you have complex problems, there probably are no simple cost-free solutions to them, because if there were, somebody would have [already] solved them.” [link]
Similar observation applies to eliminating fiber-dependence and related problems — it isn‘t the same as changing a fuse or replacing a circuit board, otherwise somebody would have already normalized them for you. Fiber was that “honest-to-goodness” attempt to solve this “complex problem,” but you already know its sorry outcome.
Even though our bodies are all similar at birth, they gradually transform due to self-inflicted damage, natural aging, medical interventions, and other factors. These determine the extent and complexity of your particular problems and the “costs” to eliminate them.
For these reasons I can share with you my extensive know-how and “battle-proven” tools to do the job, but you have to continuously adapt these tools and suggestions to yourself. And that means studying and understanding the “user manual,” which is what Fiber Menace and this site are.
If you do, you‘ll be rewarded with better health, an improved quality of life, and, hopefully, a much longer life. If you can‘t or are too busy, try to find an attentive doctor who can help you, hopefully without fiber and laxatives.
I am not trying to scare you off — when push comes to shove, it‘s an extremely simple approach that can be summarized in four lines:
— Cut out all sources of processed fiber.
— Normalize stools, flora, and colon function with Hydro-CM program.
— Maintain regularity to prevent large stools and/or fecal impaction.
That‘s really all there is to it. But that‘s just like playing golf — a club, a ball, and a hole. What‘s the big deal, right? But even picking the right club or hitting the center of the ball requires knowledge, patience, and hands-on training.
Obviously, having normal stools isn‘t like playing Masters at Augusta. But the more you know about it, the better you‘ll be able to manage the process and the exceptions. Once you learn the basic rules and practice a little, this will become second nature, no different than brushing your teeth.
And don‘t forget to share your knowledge with people who don‘t know about this site yet! Just one e-mail may save someone from years and years of misery and disease. In many families, anything connected to stools is a taboo subject. So parents, spouses, and adult children may silently pretend that everything is fine until the day a disaster strikes.
Don‘t ask! Don‘t presume. Just send the link to this page via e-mail or share it via Facebook, and let your friends, colleagues, and family deal with this issue in the privacy of their own computers! Tell them it‘s an interesting site about fiber, and they‘ll figure out the rest!
Konstantin Monastyrsky
If you are experiencing abdominal pain, rectal bleeding, tarry stools, diarrhea, dehydration, fecal impaction, acute diverticulosis, or haven't had bowel movements over a three-day period, visit your doctor or emergency room immediately. DO NOT DO ANYTHING described here or in author's book!
The information presented here is educational in nature, represents the author‘s opinion and experience, and isn‘t intended to treat, cure, prevent, and diagnose any disease. The author is not a medical doctor. Before changing your diet and taking supplements, consult your doctor or pharmacist to make sure they will not interfere with any medical treatment you may be undergoing.